
6I2,
I72.2
THE
RELATION
BETWEEN
AMPLITUDE
OF
CONTRACTION
AND
RATE
OF
RHYTHM
IN
THE
MAMMALIAN
VENTRICLE.
(INCLUDING
INTERPRE-
TATION
OF
THE
APPARENT
INDIRECT
ACTION
OF
THE
VAGUS
ON
AMPLITUDE
OF
VENTRICULAR
CONTRACTION
.)1
By
ALISON
S.
DALE.
(From
the
Physiological
Laboratory,
Cambridge.)
PART
I.
THE
APPARENT
INDIRECT
ACTION
OF
THE
VAGUS
ON
THE
AMPLITUDE
OF
VENTRICULAR
CONTRACTION.
Introductory.
THE
question
whether
the
ventricle
of
the
mammalian
heart
receives
inhibitory
fibres
from
the
vagus
nerve
has
produced
much
conflicting
evidence.
It
is
a
well-established
fact,
that,
after
complete
dissociation
between
auricle
and
ventricle
has
been
produced
by
crushing
or
cutting
of
the
A.-v.
bundle
[Krehl
and
Romberg,
1892;
Hering,
1905;
Erlanger,
1909],
stimulation
of
the
vagus
nerve
has
no
effect
on
the
rhythm
of
the
ventricle
or
on
the
strength
of
its
contractions.
Injection
of
vago-mimetic
drugs,
however,
still
produces,
in
the
rabbit,
a
slight
slowing,
suggesting
a
weak
negative
chronotropic
action
of
the
vagus
on
the
ventricle
itself
[Krehl
and
Romberg,
1892;
Cullis
and
Tribe,
1913],
though
the
distribution
of
the
fibres
concerned
is
unknown.
With
regard
to
the
inotropic
action
of
the
vagus
on
the
ventricle
the
evidence
is
conflicting.
Cullis
and
Tribe
showed
that,
in
the
per-
fused
intact
heart
in
situ,
stimulation
of
the
vagus
nerve
or
injection
of
vago-mimetic
drugs
slowed
the
heart
rhythm,
and
at
the
same
time
decreased
the
strength
of
contraction
of
both
auricle
and
ventricle.
When
the
bundle
was
cut
the
effects
on
the
ventricle
of
stimulating
the
nerve
and
of
injection
of
drugs
were
abolished,
except
for
the
slight
slowing
1
This
work
was
carried
out
during
the
tenure
of
the
Gilchrist
Studentship
of
Newnham
College,
and
the
Michael
Foster
Studentship
of
the
University
of
Cambridge.

A.
S.
DALE.
produced
by
relatively
large
doses.
More
recent
work
by
Drury
[1923]
and
Rothberger
and
Scherf
[1930]
on
the
whole
animal
(dog)
has
shown
that,
if
the
ventricular
rate
is
maintained
constant
by
rhythmic
shocks
throughout,
vagus
stimulation
does
not
influence
the
strength
of
the
ventricular
contractions.
Cullis
and
Tribe,
finding
that
the
vagus
or
vago-mimetic
drugs
only
affected
the
strength
of
contraction
of
the
ventricle
when
the
latter
was
connected
to
the
auricle
by
the
A.-V.
bundle,
concluded
that
"normally,
the
vagus
exerts
its
effect
on
the
ventricle,
only
indirectly,
through
its
action
on
the
auricular
rhythm."
The
present
experiments
were
carried
out
in
an
attempt
to
determine
what
the
nature
of
this
"indirect"
action
might
be.
Methods.
The
experiments
were
performed,
with
one
exception,
on
the
hearts
of
rabbits.
In
the
one
exception
a
cat's
heart
was
used.
The
animals
were
killed
by
a
blow
on
the
head
and
the
hearts,
after
removal
from
the
body,
were
perfused
with
a
modified
Ringer's
solution
by
means
of
a
cannula
tied
into
the
aorta.
The
cannula
carried
a
thermometer,
and
the
solution
entered
by
a
side
tube.
The
perfusion
pressure,
which
was
about
1
metre
of
saline,
was
maintained
from
a
Mariotte's
bottle,
suspended
at
a
suitable
height.
From
the
Mariotte's
bottle
the
solution
passed
to
a
glass
tower
where
oxygen
was
continuously
bubbled
through
it,
and
thence
to
a
glass
coil
immersed
in
a
water
bath.
The
coil
was
connected
by
rubber
tubing
to
the
side
tube
of
the
cannula.
The
temperature
in
the
water
bath
was
regulated
so
that
the
thermometer
in
the
cannula
registered
36-380
C.
The
composition
of
the
Ringer's
solution
was
as
follows:
NaCl
0-85
p.c.,
Na2HPO4
0-06
p.c.,
KCI
0-042
p.c.,
dextrose
0.1
p.c.,
CaCl2
0x024
p.c.
The
pH
was
adjusted
to
7x5
by
the
addition
of
HCI,
comparison
being
made
with
a
standard
buffer
solution,
using
phenol
red
as
indicator.
The
water
used
in
making
up
the
solution
was
distilled
in
a
porcelain
still.
Great
difficulty
was
experienced
initially
as,
although
the
auricles
beat
quite
vigorously,
the
ventricles
contracted
only
very
feebly
or
not
at
all.
This
was
found
to
be
due
to
the
presence
in
the
distilled
water
of
a
high
concentration
of
CO2.
If
the
water,
after
condensation,
was
thoroughly
boiled
and
allowed
to
cool
before
use
the
hearts
beat
very
well.
It
was
found
later
that
this
precaution
of
using
boiled
water
for
the
solution
was
only
necessary
at
the
beginning
of
an
experiment.
When
the
heart
was
once
beating
vigorously,
solution
containing
C02
could
be
used
without
having
any
deleterious
effect.
The
reason
for
this
effect
of
002
456

HEART
RATE
AND
SIZE
OF
CONTRACTION.
is
not
understood,
but
it
would
seem
to
be
specific
and
not
due
to
its
acid
properties,
as
the
reaction
of
the
solution
was
always
controlled.
The
drug
used
in
most
of
the
experiments
was
arecoline,
though
acetylcholine
was
occasionally
used.
The
latter
is
not
very
satisfactory
in
these
experiments,
however,
as
its
effect
is
too
transient.
The
arecoline
was
obtained
as
the
crystalline
bromide
and
made
up
in
a
0-1
p.c.
solution.
This
was
diluted
with
Ringer's
solution
to
0.001
p.c.
for
each
experiment.
The
usual
dose
was
0-1
c.c.
to
0-5
c.c.
of
this
diluted
solution,
injected
with
a
syringe
into
the
rubber
tubing
leading
to
the
cannula.
The
contractions
of
the
left
auricle
and
left
ventricle
were
recorded
by
means
of
light
straw
levers
carrying
B
ayli
ss
writing
points.
The
levers
were
held
in
brass
bearings,
and
the
vibration
frequency
of
each
was
increased
by
a
small
rubber
band
which
resisted
the
raising
of
the
lever.
The
heart
was
suspended
vertically
from
the
cannula,
and
the
apex
of
the
left
ventricle
was
fixed
by
a
ligature
to
a
metal
rod.
One
lever
was
attached
to
a
point
near
the
base
of
the
ventricle
by
a
silk
thread
sewn
through
the
epicardium,
the
other
to
the
left
auricular
wall
in
the
same
way.
By
this
method
of
attachment
the
use
of
pulleys
for
the
ventricular
record
is
avoided,
and
the
risk
of
distortion
of
the
record
by
movements
(swinging,
etc.)
of
the
whole
heart
is
greatly
diminished.
It
has
the
further
advantage,
of
special
importance
in
these
experiments,
that
the
shortening
of
the
ventricular
muscle
is
recorded,
uncomplicated
by
the
pull
of
the
auricular
contraction.
In
order
to
avoid
distension
of
the
left
ventricle
by
perfusion
fluid
leaking
through
the
aortic
valves,
a
glass
tube
was
passed
into
the
cavity
of
the
ventricle
through
a
small
slit
made
in
its
apex,
and
tied
in
position.
Any
fluid
tending
to
collect
in
the
ventricle
was
thus
drained
away.
Results.
Effects
of
vago-mimetic
drugs.
The
object
of
the
first
experiments
was
to
repeat
the
experiment
of
Cullis
and
Tribe.
The
effects
of
varying
doses
of
arecoline
on
the
heart
with
A.-v.
bundle
intact
were
first
recorded.
The
bundle
was
then
cut
and
the
procedure
repeated.
Fig.
1
gives
a
typical
example
of
the
records
obtained.
It
will
be
noticed
that
in
record
a,
taken
before
cutting
the
bundle,
the
injection
of
0.001
mg.
of
arecoline
is
followed
by
a
slowing
of
the
heart
rhythm,
accompanied
by
a
diminution
in
the
amplitude
of
the
auricular
and
the
ventricular
contractions.
A
curious
point
is
the
rise
of
the
base
line,
which
is
particularly
noticeable
in
the
ventricular
tracing.
The
reason
for
this
rise
is
not
clearly
understood,
but
in
any
case
it
is
457

A.
S.
DALE.
unconnected
with
the
diminution
in
the
amplitude
of
the
contractions,
as
it
occurs
after
the
bundle
is
cut,
when
no
such
diminution
is
seen.
Fig.
1.
Exp.
3.
xii.
29.
Read
from
right
to
left.
In
both
a
and
b
the
upper
tracing
is
the
ventricular
reoord,
the
lower
that
of
auricle
followed
by
ventricle.
a.
Intact
heart.
b.
After
cutting
the
bundle.
Further,
when
another
method
of
registration,
which
will
be
described
later,
is
used,
this
rise
of
the
base
line
does
not
occur,
while
the
diminution
in
the
size
of
the
ventricular
contractions
is
still
observed.
It
will
be
noticed
that
premature
contractions
are
followed
by
greatly
enlarged
ventricular
beats.
The
significance
of
this
will
be
considered
later.
Record
b
shows
the
effect
of
arecoline
after
section
of
the
A.-v.
bundle.
The
dose,
0.01
mg.,
is
sufficient
to
inhibit
the
auricular
contractions
almost
completely,
while
the
ventricular
rate
is
slightly
diminished.
A
close
scrutiny
reveals
a
very
slight
decrease
in
the
height
of
the
ven-
tricular
record,
but
this
decrease
is
very
much
smaller
than
that
observed
before
cutting
the
A.-v.
bundle.
The
results
just
described,
which
are
typical
of
many
obtained,
are
identical
with
those
of
Cullis
and
Tribe,
except
for
one
small
difference.
Cullis
and
Tribe
never
obtained
a
diminution
in
amplitude
of
the
ventricular
contractions
when
vago-
mimetic
drugs
were
injected
after
section
of
the
A.-v.
bundle.
In
the
458

HE"ART
RATE
AND
SIZE
OF
CONTRACTION.
present
experiments
this
diminution
was
only
obtained
with
large
doses
of
arecoline.
Normal
doses
had
no
such
effect.
Cullis
and
Tribe's
conclusion
still
holds,
therefore,
for
normal
doses,
while
for
large
doses
we
may
qualify
it
by
adding
that
arecoline
affects
the
size
of
the
ven-
tricular
contractions
greatly
when
the
A.-V.
bundle
is
intact,
and
slightly
when
the
ventricle
is
no
longer
in
connection
with
the
auricle.
With
regard
to
the
nature
of
this
"indirect"
action,
it
might
be
supposed
that
the
diminution
in
the
size
of
the
ventricular
contractions
was
due
to
a
change
in
the
impulse
passing
by
the
A.-v.
bundle
from
auricle
to
ventricle.
If
that
were
the
case
the
phenomenon
would
present
a
clear
exception
to
the
"All
or
None"
law.
Such
a
supposition,
however,
is
unnecessary,
as
a
much
simpler
explanation
is
at
hand.
Close
inspection
of
the
records
of
the
present
series
of
experiments
shows
that
the
ventricular
contrac-
tions
only
decreased
in
size
after
injection
of
arecoline
when
the
heart
rhythm
was
slowed,
which
suggested
that
the
change
of
rate
is
in
some
way
responsible
for
the
change
in
the
size
of
the
contractions.
This
is
supported
by
the
fact
that
the
idio-ventricular
rhythm
which
obtains
after
section
of
the
A.-V.
bundle
is
only
slightly
influenced
by
arecoline,
and
that
in
the
ventricle
isolated
in
this
manner
the
size
of
the
beat
remained
unchanged
by
any
dose
of
arecoline
which
did
not
affect
the
rate.
It
is
evident
that
if
the
diminution
in
the
amplitude
of
the
ven-
tricular
contractions,
which
follows
injection
of
arecoline
when
the
bundle
is
intact,
is
simply
due
to
the
slowing
of
the
rhythm,
then
a
similar
diminution
should
occur
when
the
rhythm
is
slowed
by
any
other
means.
Effects
of
cooling
the
S.-A.
node.
A
series
of
experiments
was,
therefore,
performed
in
which
the
heart
rate
was
decreased
by
cooling
of
the
S.A.
node.
The
preparation
was
set
up
as
before,
and
the
cooling
was
effected
by
means
of
a
piece
of
narrow
lead
pipe
through
which
iced
water
flowed.
The
pipe
was
bent
sharply
at
one
point,
and
the
outer
surface
of
the
bend
was
brought
into
contact
with
the
region
of
the
S.-A.
node,
thus
producing
localized
cooling.
Fig.
2a
shows
a
typical
example
of
the
result
of
slowing
the
rhythm
by
this
method;
b
and
c
show
the
effect
of
two
different
doses
of
arecoline
for
comparison.
In
c
a
2-1
block
was
produced
by
the
drug,
the
ventricular
rhythm
thus
slowing
to
about
the
same
degree
as
that
produced
by
cooling
in
a,
and
it
will
be
seen
that
the
diminution
in
the
size
of
the
ventricular
contractions
is
prac-
tically
the
same
in
the
two
cases.
Effects
of
drugs
at
constant
rhythms.
Such
results
give
very
strong
support
to
the
hypothesis
that
the
slowing
of
the
rhythm
is
the
deter-
459

mining
factor
in
the
action
of
arecoline
on
the
size
of
the
ventricular
contractions
in
the
intact
heart.
It
now
remained
to
be
determined
Fig.
2.
Exp.
13.
xii.
29.
Read
from
right
to
left.
In
a,
b
and
c
upper
tracing
represents
auricular
followed
by
ventricular
contractions.
Lower
tracing
ventricular
contractions
only.
a.
S.-A.
node
cooled
between
points
indicated
by
arrows.
b.
0002
mg.
arecoline
injected
shortly
before
beginning
of
record.
c.
0005
mg.
arecoline
injected
shortly
before
beginning
of
record.
Arrow
indicates
beginning
of
2-1
block.
whether
the
size
of
ventricular
contractions
would
be
unaffected
by
arecoline
when
the
heart
rate
was
maintained
artificially
constant.
The
heart
was,
therefore,
stimulated
rhythmically
by
electrodes
placed
on
the
right
auricle.
The
rhythmic
shocks
were
produced
by
means
of
a
rotary
contact
breaker
placed
in
the
primary
circuit
of
an
induction
coil.
Fig.
3
shows
the
results
of
such
an
experiment,
and
includes
a
record
of
slowing
by
cooling
for
comparison.
Fig.
3
a
shows
the
usual
result
of
cooling
the
S.-A.
node:
b
shows
the
A.
S.
DAlB.
460

HEART
RATE
AND
SIZE
OF
CONTRACTION.
461
effect
of
injecting
a
small
dose
of
arecoline
while
the
heart
was
being
driven
at
constant
rate.
The
dose
0002
mg.
is
one
which,
with
spontaneous
Fig.
3.
Exp.
11.
ii.
30.
Read
from
left
to
right.
In
a,
b
and
c.
Upper
tracing
represents
auricular
followed
by
ventricular
contractions.
Auricular
contractions
are
smaller
than
ventricular,
but
their
height
can
be
seen
as
the
upper
edge
of
the
denser
portion
of
the
tracing.
Lower
tracing
is
that
of
ventricular
contractions
only.
a.
Cooling
of
S.-A.
node.
Auricular
tracing
disappears
owing
to
substitution
of
nodal
for
sinus
rhythm.
b.
Heart
driven
at
constant
rate.
Injection
of
0'002
mg.
arecoline
at
arrow.
c.
Heart
driven
at
constant
rate.
Injection
of
0
005
mg.
arecoline
at
first
arrow.
Second
arrow
indicates
appearance
of
2-1
block.
rhythm,
would
produce
a
marked
slowing,
with
weakening
of
the
ven-
tricular
contraction.
In
this
case
the
strength
of
contraction
is
unaffected.
Record
c
provides
especially
clear
evidence
on
the
point
under
discussion.
The
dose
was
a
large
one,
0005
mg.,
which
almost
abolished
the
auricular
contractions
at
one
point.
Later,
when
the
auricular
beats
were
re-
PH.
LXX.
30
A.
S.
DALE.
covering,
the
effect
on
the
A.-V.
conducting
system
became
evident,
and
a
2-1
block
was
produced.
The
amplitude
of
the
ventricular
contrac-
tions,
which
till
then
had
remained
unchanged,
immediately
diminished
in
size,
and
this
reduction
of
amplitude
persisted
as
long
as
the
2-1
block
was
maintained.
The
period
of
block
was
followed
by
a
short
phase
in
which
an
occasional
beat
was
dropped.
After
this
the
block
disappeared
completely,
a
ventricular
contraction
following
each
auricular
one,
and
with
this
resumption
of
the
original
rhythm
by
the
ventricle,
the
con-
tractions
returned
to
their
normal
size.
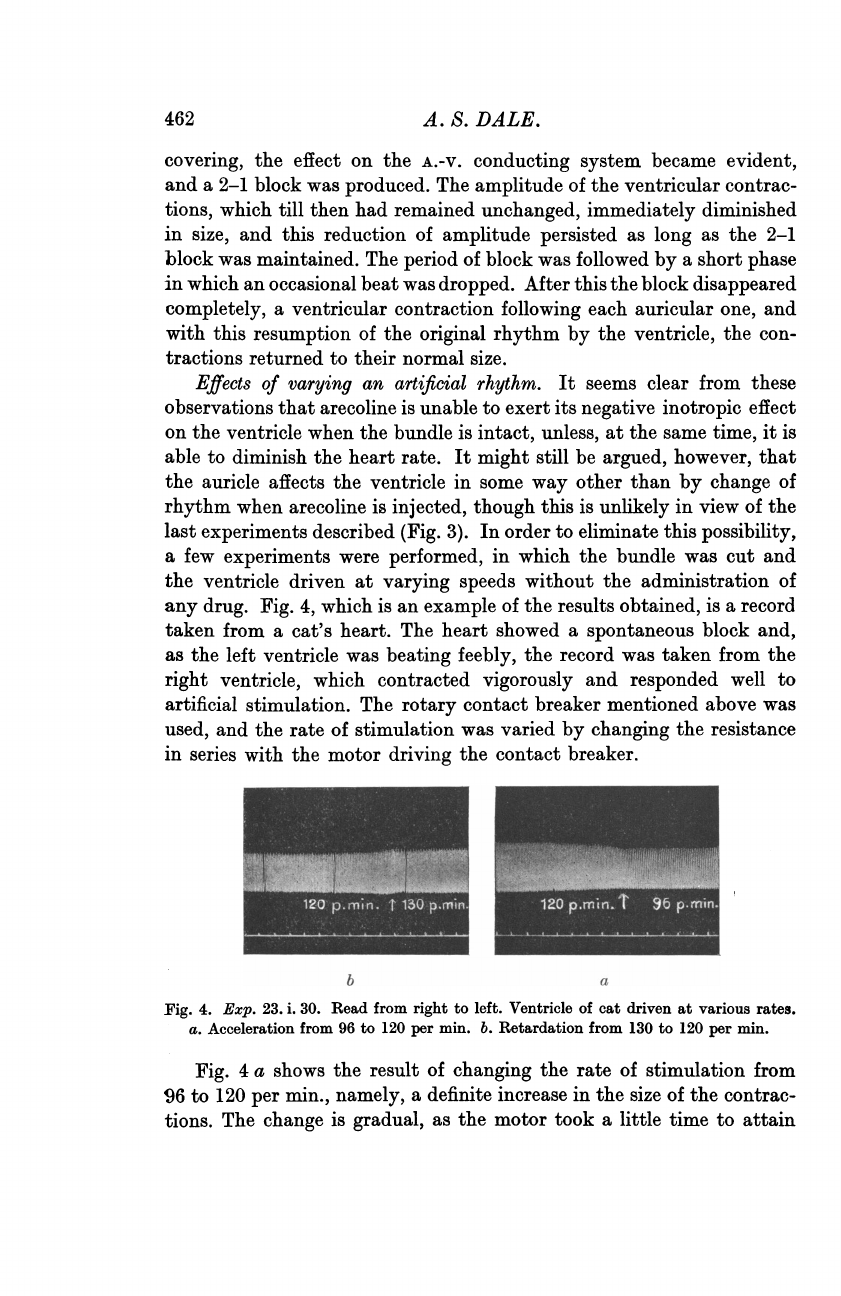
Effects
of
varying
an
artificial
rhythm.
It
seems
clear
from
these
observations
that
arecoline
is
unable
to
exert
its
negative
inotropic
effect
on
the
ventricle
when
the
bundle
is
intact,
unless,
at
the
same
time,
it is
able
to
diminish
the
heart
rate.
It
might
still
be
argued,
however,
that
the
auricle
affects
the
ventricle
in
some
way
other
than
by
change
of
rhythm
when
arecoline
is
injected,
though
this
is
unlikely
in
view
of
the
last
experiments
described
(Fig.
3).
In
order
to
eliminate
this
possibility,
a
few
experiments
were
performed,
in
which
the
bundle
was
cut
and
the
ventricle
driven
at
varying
speeds
without
the
administration
of
any
drug.
Fig.
4,
which
is
an
example
of
the
results
obtained,
is
a
record
taken
from
a
cat's
heart.
The
heart
showed
a
spontaneous
block
and,
as
the
left
ventricle
was
beating
feebly,
the
record
was
taken
from
the
right
ventricle,
which
contracted
vigorously
and
responded
well
to
artificial
stimulation.
The
rotary
contact breaker
mentioned
above
was
used,
and
the
rate
of
stimulation
was
varied
by
changing
the
resistance
in
series
with
the
motor
driving
the
contact
breaker.
I
a
Fig.
4.
Exp.
23.
i.
30.
Read
from
right
to
left.
Ventricle
of
cat
driven
at
various
rates.
a.
Acceleration
from
96
to
120
per
min.
b.
Retardation
from
130
to
120
per
min.
Fig.
4
a
shows
the
result
of
changing
the
rate
of
stimulation
from
96
to
120
per
min.,
namely,
a
definite
increase
in
the
size
of
the
contrac-
tions.
The
change
is
gradual,
as
the
motor
took
a
little
time
to
attain
462

HEART
RATE
AND
SIZE
OF
CONTRACTION.
the
new
speed.
Fig.
4
b
shows
the
change
in
the
reverse
direction,
from
130
to
120
per
min.,
the
result
being
a
diminution
in
the
size
of
the
contractions.
It
will
be
noticed
that
the
size
of
the
contractions
at
130
per
min.
in
record
b
is
smaller
than
that
at
120
per
min.
in
record
a.
This
is
probably
a
fatigue
effect,
since,
when
the
rate
was
increased
from
120
to
130
per
min.,
there
was
an
increase
in
the
size
of
the
contractions
at
first,
but
this
gave
way
to
a
gradual
diminution.
It
seems
probable
that
the
heart
could
not
maintain
such
a
vigorous
contraction
at
this
high
rate
when
depending
only
on
the
oxygen
dissolved
in
the
Ringer's
solution.
When
the
stimulation
rate
was
reduced
again
to
96
per
min.
the
contractions
gradually
regained
their
original
size
corresponding
to
this
rate.
It
is
possible,
therefore,
to
vary
the
size
of
the
ventricular
contraction
by
changing
the
rhythm,
when
this
is
being
produced
artificially,
in
exactly
the
same
way
as
when
the
ventricle
is
receiving
its
stimuli
from
the
auricle
by
way
of
the
A.-v.
bundle.
Experiments
with
perfused
ventricular
strips,
to
be
described
later,
confirm
this.
A
point
which
is
important
for
later
discussion
must
be
mentioned
here.
It
is
evident
in
all
curves
in
which
there
is
an
abrupt
slowing
of
the
heart-rate,
that
the
beat
following
the
first
prolonged
pause
is
en-
larged,
and
that
this
is
then
followed
by
a
descending
staircase
of
beats,
until
the
small
size
of
beat,
typical
of
the
slower
rate,
is
reached.
The
change
from
slow
to
fast
rate
is
usually
more
gradual,
but
where
an
abrupt
change
occurs,
as
in
Fig.
2
c,
where
a
2-1
block
gives
way
to
the
normal
A.-V.
sequence,
it
is
evident
that
the
beat
following
the
first
short
pause
is
diminished,
and
is
followed
by
an
ascending
staircase
of
beats.
Demonstration
of
effect
in
tension
records.
From
the
results
of
the
experiments
so
far
described
it
must
be
concluded
that,
in
the
isolated
perfused
rabbit's
heart
in
which
the
contractions
are
recorded
by
means
of
levers,
the
so-called
indirect
effect
of
vago-mimetic
drugs
on
the
size
of
the
ventricular
contractions
is
due
to
the
slowing
of
the
rhythm
produced
by
the
action
of
the
drug
on
the
pacemaker
of
the
heart.
Experiments
with
levers,
however,
are
always
open
to
criticism
on
the
ground
that
distortioA
of
the
records
may
occur,
owing
to
the
natural
vibration
frequency
of
the
levers
being
too
low.
In
the
case
of
a
rapidly
beating
rabbit's
heart
it
is
essential
that
the
recording
system
have
a
high
natural
frequency,
and
it
might
well
be
argued
that,
in
the
experi-
ments
above
described,
the
excursions
of
the
lever
give
a
true
record
of
the
size
of
the
contractions
only
when
the
rate
is
slow,
the
larger
excursions
at
higher
rates
of
beating
being
due
to
overthrow
of
the
lever.
30-2
463

In
order
to
eliminate
such
an
objection
the
experiments
were
repeated,
using
a
high-frequency
system
for
recording
the
tension
changes
in
the
ventricular
muscle.
Fig.
5.
Diagram
of
apparatus
for
recording
intraventricular
pressure.
a,
brass
tube
carrying
membrane;
b,
rubber
membrane
with
mirror
attached
radially;
c,
connecting
tube
of
lead
piping;
d,
brass
tube
to
which
balloon
e
is
attached;
f,
5
c.c.
pipette
containing
liquid
paraffin
for
filling
balloon;
A
and
B,
3-way
(T)
taps.
Fig.
5
is
a
diagrammatic
representation
of
the
apparatus
used.
It
consisted
essentially
of
a
balloon,
filled
with
fluid
which
was
introduced
into
the
cavity
of
the
left
ventricle,
and
connected
by
tubes
filled
with
fluid
to
a
tightly
stretched
rubber
membrane.
A
mirror
attached
to
the
membrane
reflected
a
beam
of
light
into
a
moving
paper
camera.
Diffi-
culty
was
experienced
at
first
in
the
choice
of
a
suitable
balloon.
Small
thin
rubber
balloons
were
tried
but,
unless
these
were
blown
to
extreme
tightness,
the
contraction
of
the
ventricle
caused
the
top
of
the
balloon
to
bulge
into
the
auricular
cavity.
In
the
process
of
this
bulging
a
large
amount
of
distortion
of
the
record
could
occur.
A
tightly
stretched
rubber
balloon
has
two
disadvantages,
the
first
that
it
bursts
very
easily,
464
A.
S.
DAlE.

HEART
RATE
AND
SIZE
OF
CONTRACTION.
and
the
second
that
the
initial
pressure
is
so
high
that
the
ordinary
glass
taps
cannot
stand
it,
and
leakages
occur.
It
was
decided,
therefore,
to
use
an
inextensible
balloon,
and
for
this
purpose
the
gall
bladder
of
a
small
cat
served
very
well.
The
bladder
was
removed
from
the
animal
and
washed
out
with
saline.
It
was
then
bound
firmly
to
a
small
piece
of
brass
tube,
and
stored
in
saline,
covered
with
a
layer
of
toluene
to
keep
it
sterile.
When
in
use
the
bladder
was
filled
with
liquid
paraffin.
Saline
is
unsuitable
as
it
diffuses
through
the
walls
of
the
bladder
when
this
is
subjected
to
pressure.
The
perfusion
apparatus
was
the
same
as
that
used
in
the
experiments
already
described.
The
bladder
was
intro-
duced
through
a
small
slit
in
the
apex
of
the
left
ventricle,
this
being
done
as
follows.
The
bladder
and
brass
tube
were
filled
with
paraffin
by
means
of
a
fine
glass
pipette,
care
being
taken
to
exclude
all
air
bubbles.
The
5
c.c.
pipette
(Fig.
5,f)
was
also
filled
with
paraffin
and
placed
in
position.
The
taps
A
and
B
were
then
turned
so
that
the
paraffin
flowed
from
the
pipette
(i)
and
filled
the
tubes
and
the
rubber
con-
a
nection
for
the
brass
tube
carrying
the
bladder.
The
brass
tube
was
then
in-
(ij)
serted
into
the
rubber
connection,
care
again
being
taken
to
avoid
the
entrance
of
air
bubbles.
The
paraffin
was
then
sucked
back
into
the
pipette,
and
the
(i)
balloon,
which
was
quite
flexible,
was
thus
inverted
into
the
brass
tube.
The
b
end
of
the
tube
could
now
easily
be
(ii)
inserted
into
the
ventricle,
and
was
tied
firmly
in
place.
Finally,
by
blowing
FiE
from
the
end
of
the
pipette,
the
bladder
was
everted
into
the
ventricular
cavity,
and
filled
to
any
desired
extent.
It
was
then
connected
with
the
membrane
by
turning
the
tap
B.
The
observations
repeated
with
this
method
of
recording
were:
cooling
of
I
the
S.-A.
node,
simple
injection
of
areco-
line,
and
injection
of
arecoline
while
the
heart
was
being
driven
at
constant
rate.
JVyA.J.
/\.A
I.
.
g.6.
Read
from
left
to
right.
Sample
curves
taken
from
two
experiments.
z.
From
Exp.
3.
v.
30.
b.
From
Exp.
6.
v.
30.
a
(i).
On
left,
heart
beating
at
normal
rhythm.
On
right,
luring
cooling
of
S.-A.
node.
a
(ii).
On
left,
heart
beating
at
normal
rhythm.
On
right,
after
injection
of
)0001
mg.
arecoline.
b
(i).
On
left,
ieart
beating
at
normal
rhythm.
)n
right,
after
injection
of
0-002
mg.
Lrecoline.
b
(ii).
On
left,
heart
driven
Lt
constant
rhythm.
On
right,
after
njection
of
0-003
mg.
arecoline.
A
2-1
block
has
appeared
and
ven-
ricular
rate
is
halved.
Fig.
6
shows
a
series
of
records,
taken
from
two
experiments,
illustrating
the
three
methods
of
slowing.
465

A.
S.
DALE.
It
is
evident
from
these
records
that
the
decreased
size
of
ventricular
contraction
produced
by
slowing
of
the heart
rhythm
is
not
an
apparent
one,
due
to
defects
in
the
recording
apparatus,
but
a
real
one,
as
it
still
persists
in
records
taken
with
an
apparatus
in
which
all
possibility
of
overthrow
is
eliminated.
The
rise
of
the
base
line
during
the
action
of
arecoline,
so
evident
in
the
records
taken
with
the
levers,
is
entirely
absent
in
these
records,
and
may
be
taken
to
be
an
artefact
peculiar
to
the
method
of
registration.
Conclusionsfrom
Part
I.
The
conclusions
to
be
drawn
from
the
experiments
described
in
Part
I
of
this
paper
may
be
summarized
as
follows:
The
results
of
other
workers,
which
show
that
vago-mimetic
drugs
such
as
arecoline,
in
small
doses,
only
influence
the
size
of
the
ventricular
contraction
when
the
A.-v.
bundle
is
intact,
have
been
confirmed.
It
has
further
been
shown
that
this
decrease
in
amplitude
is
a
real
one,
and
is
not
produced
by
imperfect
methods
of
registration.
That
the
effect
is
only
observed
when
the
ventricle
is
connected
with
the
auricle
is
due
to
the
fact
that,
in
this
case,
the
heart
rhythm
is
greatly
slowed
by
the
drugs
in
question,
whereas
the
idio-ventricular
rhythm,
which
sets
in
after
bundle
section,
is
only
affected
to
a
very
small
degree.
The
theory
that
it
is
the
slowing
of
the
rhythm
which
determines
the
diminished
size
of
the
ventricular
contractions
is
supported
by
the
facts
that
the
drug
does
not
affect
the
ventricle
when
the
heart
rate
is
kept
constant
by
rhythmic
auricular
stimulation,
and
that
when
the
dose
is
large
enough
to
produce
heart
block,
the
slowing
of
the
ventricular
rhythm
which
results
produces
a
diminution
in
the
size
of
the
contrac-
tions.
Further,
a
slowing
of
the
rhythm
produced
by
cooling
of
the
S.-A.
node
produces
effects
on
the
ventricle
identical
with
those
observed
after
injection
of
arecoline.
That
the
inotropic
effect
is
truly
secondary
to
the
chronotropic
effect,
and
does
not
depend
on
some
obscure
auricular
influence,
is
shown
by
the
fact
that
it
can
be
produced
in
the
isolated
ventricle
when
this
is
stimulated
artificially
and
the
rate
of
stimulation
is
varied.
466

HEART
RATE
AND
SIZE
OF
CONTRACTION.
PART
II.
THE
RELATION
BETWEEN
AMPLITUDE
OF
CONTRACTION
AND
RATE
OF
RHYTHM.
The
relation
between
the
rate
of
beating
and
size
of
contraction
which
has
been
described
in
Part
I
is
not
the
generally
accepted
one.
For
the
mammalian
heart,
at
least,
it
is
usually
stated
that
the
con-
tractions
are
more
vigorous
at
slow
rates
than
at
fast
ones,
the
customary
explanation
being
that
at
the
slow
rates
the
muscle
has
more
time
for
recovery
between
beats.
The
fact
that
the
relation
so
stated
is
the
exact
opposite
of
that
described
in
Part
I
of
this
paper
must
be
due
to
dif-
ferences
in
experimental
method.
There
appear
to
be
two
methods
of
experiment
in
which
increased
amplitude
with
slowing
of
the
rhythm
would
be
observed.
The
first
is
that
in
which
the
whole
animal
is
employed,
and
the
heart
is
left
in
situ.
Slowing
of
the
rhythm,
produced,
for
example,
by
cooling
of
the
S.-A.
node,
will
allow
increased
time
for
filling
of
the
ventricles
during
diastole
with
consequent
greater
length
of
ventricular
fibres
at
the
beginning
of
systole.
The
second
method
uses
the
isolated
perfused
heart,
in
which
slowing
of
the
rhythm
is
produced
by
cooling
of
the
perfusion
fluid.
In
this
way,
not
only
is
the
pacemaker
cooled,
thus
slowing
the
rhythm,
but
the
ventricular
muscle
is
also
cooled.
Cooling
of
the
heart
muscle
is
known
to
produce
larger
con-
tractions,
even
when
the
heart
rate
is
kept
constant.
To
account
for
the
smaller
contractions
at
slower
rates,
observed
in
the
present
series
of
experiments,
two
possibilities
offer
themselves.
A
simple
and
easily
tested
hypothesis
is
based
on
Wiggers'
theory
of
fractionate
contractions.
It
is
quite
conceivable
that,
at
slow
rates,
the
impulse
would
travel
more
slowly,
so
that
fewer
muscular
fractions
would
be
in
action
at
any
one
moment,
and
the
records
would
show
curves
which
were
smaller
in
height,
but
proportionately
greater
in
duration,
than
those
found
at
high
rates.
The
other
possibility
is
that
the
phenomenon
is
a
property
of
the
cardiac
muscle
itself.
(1)
The
former
hypothesis
was
tested
first.
If
it
were
correct,
then
the
duration
of
a
contraction
should
always
show
a
distinct
increase
at
the
slower
rates.
The
measurements
were
made
on
the
optical
records
which
had
been
taken
on
fast
moving
paper
(see
Fig.
6).
In
many
cases
the
decrease
of
amplitudes
with
decrease
of
rate
was
accompanied
by
no
increase
in
duration.
In
a
few
cases
the
duration
showed
a
slight
increase
under
these
conditions;
but
this
was
never
great
enough
to
467

account
for
decrease
of
amplitude
by
slowing
of
transmission,
and
in
many
cases,
notably
those
in
which
arecoline
was
used,
the
slight
increase
of
duration
persisted
after
return
to
the
original
rhythm
and
amplitude.
It
cannot,
therefore,
be
connected
with
the
slowing
of
rhythm
and
loss
of
amplitude,
and
is
probably
a
fatigue
effect
due
to the
filling
of
the
ventricular
cavity
with
the
tense
bladder.
An
unlikely
possibility
still
remained,
namely,
that
at
the
slower
rates
the
impulse
might
travel
by
a
different
path,
and
so
alter
the
shape
and
size
of
the
ventricular
mechanogram.
Rothberger
and
Scherf
[1930]
showed
that
a
change
in
the
point
of
application
of
artificial
stimuli
to
the
ventricle
in
the
whole
animal,
changed
both
the
electro-
cardiogram
and
the
intra-ventricular
pressure
curve.
To
test
this
possi-
bility,
electrical
records
were
taken'.
The
hearts
were
set
up
for
perfusion
in
the
usual
way,
and
simultaneous
records
were
taken
of
the
electro-
cardiogram
and
the
tension
developed
by
the
ventricular
muscle,
the
latter
by
the
balloon
method
already
described.
Slowing
was
produced
by
cooling
of
the
S.-A.
node,
and
by
injection
of
acetylcholine.
Arecoline
is
unsuitable
for
these
observations,
as
it
produces
permanent
changes
in
the
form
of
the
electrocardiogram,
especially
in
the
T-wave,
which
persist
after
the
effect
on
the
mechanogram
has
disappeared.
Measure-
ment
of
the
records
showed
that,
when
slowing
of
the
heart
rate
was
produced
by
cooling
the
S.-A.
node
or
injecting
acetylcholine,
with
a
corresponding
diminution
of
amplitude,
in
many
cases
the
electro-
cardiogram
was
unchanged.
In
some
there
was
a
slight
alteration
in
the
T-wave,
but
in
no
case
was
there
any
change
in
the
initial
QRS
complex,
which
is
determined
by
the
spread
of
the
excitatory
process.
These
experiments
rule
out
the
possibility
that
the
smaller
contractions
at
slow
rates
are
due
to
changes
in
the
rate
or
the
path
of
propagation
of
the
impulse.
(2)
It
seemed
probable,
accordingly,
that
the
phenomenon
was
due
to
a
property
of
the
cardiac
muscle
itself,
and,
to
test
this,
experiments
were
carried
out
on
perfused
ventricular
strips.
Rabbits'
hearts
were
used
as
before.
Strips
of
rabbits'
ventricle
have
the
advantage
that
they
do
not
beat
spontaneously,
so
that
no
difficulty
was
experienced
in
imposing
artificial
rhythms
on
them.
Fig.
7
gives
a
diagrammatic
representation
of
the
apparatus
used.
The
Ringer's
solu-
tion
was
of
the
same
composition
as
that
used
in
the
experiments
on
the
whole
heart,
and
the
arrangements
for
oxygenating
and
warming
it
were
the
same
as
before.
The
cannula,
a
glass
tube
bent
twice
at
right
angles,
1
I
am
much
indebted
to
Dr
A.
N.
Drury
for
his
help
in
the
taking
of
these
records.
A.
S.
DALE.
468

HEART
RATE
AND
SIZE
OF
CONTRACTION.
was
drawn
out
into
a
nozzle,
sufficiently
fine
for
insertion
into
one
of
the
coronary
arteries
through
its
opening
out
of
the
aorta.
A
silk
ligature,
g
coiL
Fig.
7.
Apparatus
for
perfusing
isolated
ventricular
strips.
a,
strip
of
ventricular
muscle;
b,
stimulating
electrodes;
c,
recording
lever
(only
part
shown).
passed
under
the
coronary
artery
with
a
curved
needle,
served
to
tie
the
nozzle
of
the
cannula
firmly
in
position.
Strips
of
right
ventricle
were
tried
at
first,
as
it
was
expected
that
they
would
survive
better;
but
it
was
found
that
the
left
ventricle
was
preferable,
probably
owing
to
the
fact
that
the
left
coronary
artery
is
the
larger,
and
allows
a
bigger
flow
of
perfusion
fluid.
In
any
case,
the
flow
was
never
large
enough
to
maintain
the
temperature
of
the
muscle
much
above
room
temperature.
It
was,
therefore,
necessary
to
immerse
the
strip
in
a
bath
of
the
Ringer's
solution.
This,
in
turn,
was
immersed
in
a
beaker
of
water,
warmed
to
the
desired
temperature
by
a
micro-burner.
The
free
end
of
the
strip
was
attached
by
a
silk
thread
to
a
lever,
similar
to
those
used
in
the
first
experiments
on
whole
hearts.
The
strip
was
stimulated
rhythmically,
one
of
the
electrodes
dipping
in
the
bath
of
Ringer's
solution,
and
the
other
being
attached
to
the
upper
free
end
of
the
strip.
The
latter
electrode
was
made
of
fine
wire
and
the
lead
from
it
was
coiled,
so
that
it
was
freely
movable,
and
did
not
impede
the
movement
of
the
strip.
The
rhythmic
stimuli
were
produced
by
means
of
a
rotary
contact
breaker,
similar
to
that
used
in
previous
experiments,
but
having
two
rotating
arms
connected
in
parallel
in
the
primary
circuit
of
an
induction
coil.
Either
arm
could
thus
complete
the
circuit,
and
they
were
so
469

adjusted
that
the
rhythm
of
shocks,
produced
when
both
were
in
action,
was
halved
by
cutting
one
out.
The
initial
rate
of
stimulation
was
con-
trolled
by
a
variable
resistance
included
in
series
with
the
motor
driving
the
contact
breaker.
Fig.
8.
Exp.
11.
vi.
30.
Read
from
left
to
right.
Record
obtained
with
perfused
strip
of
left
ventricle.
Stimulated
rhythmically
at
a
rate
of
50
per
min.
At
first
arrow
rate
of
stimulation
was
halved.
At
second
arrow
it
returned
to
normal.
Fig.
8
gives
a
typical
example
of
the
results
obtained.
It
will
be
noticed
that,
when
the
rate
of
the
stimulating
shocks
is
halved,
the
beat
after
the
-first
longer
pause
is
enlarged,
and
that
the
following
beats
gradually
decrease
in
size
until
a
minimum
is
reached.
When
the
original
rhythm
is
resumed
the
beat
following
the
first
shorter
interval
is
dis-
tinctly
smaller,
but,
the
following
beats
at
the
more
rapid
rhythm
gradually
increase
in
size
until
they
are
as
large
as
those
initially
pro-
duced
at
that
rate.
This
series
of
events
agrees
in
every
detail
with
what
is
observed
in
the
whole
ventricle
when
the
rhythm
is
slowed.
Another
property,
common
to
the
whole
ventricle
and
the
strips,
is
observed
when
the
slowing
of
the
rhythm
is
long
enough
maintained.
When
the
slowing
persists
for
more
than
ten
or
fifteen
beats,
it
is
noticed
that
the
size
of
the
beats
tends
again
to
increase
gradually
from
the
mnimum,
though
it
does
not
attain
the
amplitude
characteristic
of
the
faster
rate.
This
was
found
to
be
much
more
distinct
in
some
whole
hearts
than
in
others,
and
the
same
was
true
of
the
strips.
After
a
secondary
increase
of
this
kind
the
return
to
the
faster
rhythm
produced
beats
which
were
supernormal
as
compared
with
those
recorded
before
slowing
took
place.
After
a
short
period
the
beats
returned
to
the
original
amplitude.
DiSCUSSION.
The
phenomenon
described
could
be
most
simply
explained
by
as-
suming
that
the
optimal
rhythm
for
rabbit's
ventricular
muscle,
that
is,
the
rhythm
at
which
the
contractions
are
maximal,
is
a
high
one;
in
fact
that
it
is
of
the
same
order
as
the
natural
sinus
rhythm.
A
slowing
of
such
a
rhythm
would
then
cause
the
contractions
to
become
smaller.
470
A.
S.
DALE.

HEART
RATE
AND
SIZE
OF
CONTRACTION.
An
example
of
such
a
high
optimal
rhythm
is
described
by
Mines
for
the
ventricles
of
certain
elasmobranch
hearts
at
temperatures
between
200
C.
and
250
C.
The
natural
rhythm
in
this
case
was
sub-optimal,
as
acceleration
by
artificial
stimulation
augmented
the
contractions.
There
is
a
striking
difference,
however,
between
the
records
obtained
by
Mine
s
and
those
obtained
in
the
present
work
on
rabbits'
hearts.
In
Mine
s'
experiments
the
first
beat
at
the
higher
rhythm
is
augmented,
and
is
followed
by
an
ascending
staircase
of
beats,
until
the
larger
size
charac-
teristic
of
the
faster
rhythm
is
reached.
When
the
artificial
stimulation
is
stopped
and
the
rhythm
returns
to
normal
the
beats
diminish
abruptly
to
the
smaller
size
without
any
intervening
staircase.
In
the
case
of
the
mammalian
ventricle,
as
has
been
already
described,
the
first
beat
at
an
accelerated
rhythm
is
always
diminished,
and
is
then
followed
by
an
ascending
staircase
of
beats
until
the
larger
size
of
contraction
is
attained.
On
the
other
hand,
when
the
rhythm
changes
from
a
high
to
a
low
one,
the
first
beat
at
the
slow
rhythm
is
augmented
and
is
then
followed
by
a
descending
staircase
until
the
smaller
size
of
beat
charac-
teristic
of
the
slow
rhythm
is
reached.
It
seems,
therefore,
that
there
is
some
other
factor
at
work
in
the
mammalian
ventricle
which
is
the
cause
of
these
transition
phenomena.
The
high
rate
of
beating
appears
to
exert
a
favourable
influence
on
the
contractility
of
the
muscle,
and
to
leave
some
"trace
"
behind
it,
which
causes
the
first
beat
at
the
slow
rhythm
to
be
augmented.
The
augmented
beat
occurring
after
a
pre-
mature
contraction
in
the
perfused
heart
could
be
explained
in
the
same
way.
It
is
worth
noting
here
that
a
premature
contraction
occurring
during
a
phase
of
slow
rhythm
with
the
resultant
small
beats
will
cause
the
beat
following
it
to
be
augmented
to
a
size
of
the
same
order
as
that
of
the
first
beat
at
the
slow
rhythm.
This
is
well
seen
in
the
ventricular
record
of
Fig.
1
a.
The
changes
in
amplitude
which
occur
when
the
rhythm
changes
from
a
slow
to
a
fast
one
do
not
fit
in
with
a
simple
explanation
based
on
an
optimal
rhythm
hypothesis.
If
we
were
concerned
with
a
simple
case
of
a
high
optimal
rhythm,
the
first
beat
at
the
higher
rhythm
should
be
enlarged,
as
in
Mines'
experiment.
In
fact
it
is
conspicuously
diminished,
and
is
followed
by
an
ascending
staircase
of
beats.
Here
again
it
seems
that
the
higher
rate
of
beating
exerts
some
favourable
influence
on
the
cardiac
muscle.
It
seems,
therefore,
that
we
cannot
define
these
high
rhythms
as
optimal
for
the
rabbit's
ventricular
muscle
in
the
generally
accepted
sense
of
the
term.
The
large
amplitudes
observed
at
the
high
rhythms
471
A.
S.
DALE.
appear
to
depend
on
a
cumulative
action
of
the
contractions
themselves.
Such
an
action
is
very
similar
to
that
described
by
B
o
wditch
from
the
frog's
ventricle,
and
it
must
be
concluded
that
we
are
dealing
here
with
a
form
of
Bowditch
staircase.
(Woodworth
[1903]
describes
a
similar
beneficial
action
of
rapid
rhythms
on
the
perfused
ventricular
apex
of
the
dog.
He
ascribes
the
enlargement
of
the
first
contraction
at
a
slowed
rhythm
to
the
combined
effects
of
this
cumulative
action
of
the
con-
tractions
and
the
prolonged
pause.)
This
explanation
is
admittedly
inconclusive.
Until
more
experi-
mental
results
are
available
it
is
impossible
to
draw
more
definite
con-
clusions.
It
is
hoped
that
further
experiments
will
make
a
more
exact
interpretation
possible.
So
far
the
relation
between
rate
and
size
of
contraction
has
only
been
discussed
with
regard
to
the
ventricle.
It
will
be
observed,
however,
that
in
the
experiments
in
which
the
S.-A.
node
was
cooled
the
auricular
contractions
diminished
in
size
when
slowing
took
place.
Great
stress
is
not
laid
on
these
results,
as
it
is
very
probable
that
a
certain
amount
of
overthrow
occurred
in
the
recording
of
the
auricular
contractions.
However,
a
recent
paper
by
H.
Loos
[1930]
supports
the
idea
that
the
relation
does
hold
for
the
auricle.
He
finds
that
the
size
of
auricular
contraction
in
the
rabbit's
heart
is
affected
more
profoundly
by
vagus
stimulation
when
the
rhythm
is
allowed
to
slow,
than
when
the
rate
is
maintained
constant
by
artificial
stimulation.
Loos'
experiments
were
performed
on
whole
rabbits,
but
the
phenomenon
was
still
observed
when
the
venae
cavae
were
clamped,
so
that
it
is
not
determined
by
factors
relating
to
the
filling
of
the
auricle.
SUMMARY.
1.
Cullis
and
Tribe's
observation,
that
vago-mimetic
drugs
only
diminish
the
amplitude
of
contraction
of
the
rabbit's
ventricle
when
the
A.-v.
bundle
is
intact,
is
confirmed.
2.
This
action
is
shown
to
depend
on
the
fact
that
the
S.-A.
nodal
rhythm
is
slowed
by
the
action
of
the
drug,
while
the
idio-ventricular
rhythm
which
obtains
after
section
of
the
A.-v.
bundle
is
not
affected,
similar
diminutions
of
amplitude
being
observed
when
the
rhythm
is
slowed
by
other
means.
3.
A
diminution
is
also
obtained
in
the
amplitude
of
contraction
of
perfused
ventricular
strips,
stimulated
artificially,
when
the
rate
of
stimulation
is
diminished.
472

HEART
RATE
AND
SIZE
OF
CONTRACTION.
473
4.
This
relation
between
the
amplitude
of
contraction
and
the
rhythm
is
ascribed
to
a
form
of
Bowditch
staircase.
In
conclusion
I
wish
to
thank
Prof.
Bar
croft
for
permission
to
carry
out
these
experiments
in
his
laboratory,
and
Dr
Anr
e
p
for
his
advice
and
criticism.
REFERENCES.
Cullis
and
Tribe
(1913).
J.
Physiol.
46,
141.
Drury
(1923).
Heart,
10,
405.
Erlanger
(1909).
Pflueger8
Arch.
127,
77.
Hering
(1905).
Pflueger8
Arch.
108,
281.
Krehl
and
Romberg
(1892).
Arch.
exp.
Path.
Pharmak.
30,
49.
Loos
(1930).
Pflueger8
Arch.
225,
1.
Rothberger
and
Scherf
(1930).
Z.
ge8.
exp.
Med.
71,
274.
Woodworth
(1903).
Amer.
J.
Phy8iol.
8,
213.
