
Key Points
• Cannabis is the second-most common psychoactive substance (after
alcohol) used during pregnancy.
• Elements of cannabis can pass through the placenta and affect the fetus’s
development. Frequent cannabis use during pregnancy is associated
with low birth weight and is part of a cluster of risk factors related to other
adverse birth outcomes.
• There are also affects on behaviour in children and young adults, including
attention deficits, emotional disturbances, increased hyperactivity and
impulsivity, sleep disorders, and increased likelihood of substance use.
• Growing evidence from human and animal studies shows that paternal
cannabis use can also negatively affect children’s neurodevelopment.
• Elements of cannabis can pass into breastmilk during lactation, which the
infant absorbs and metabolizes.
• The effects of cannabidiol (CBD) use during pregnancy or breastfeeding
are unknown. Both clinical and preclinical studies are urgently needed to
evaluate the safety of CBD use during pregnancy.
• Information on the effects of cannabis use during pregnancy is essential to
help healthcare providers advise patients about the effect of cannabis use
and improve the health and well-being of patients and their children.
• Pregnant or breastfeeding parents should have informed discussions with
healthcare providers about the potential adverse effects of cannabis use
during pregnancy to help them better understand the potential risks and help
them make informed and healthy choices.
Clearing the Smoke
on Cannabis
Cannabis Use During Pregnancy
and Breastfeeding
– An Update
Justine Renard, Ph.D.,
Research and Policy Analyst, CCSA
Sarah Konefal, Ph.D.,
Research and Policy Analyst, CCSA
This is the second in a series of
reports that reviews the effects of
cannabis use on various aspects of
human functioning and development.
This report focuses on maternal
cannabis use during pregnancy and
breastfeeding and its effects on
children and young adults. It updates
a previous report with new research
findings that validate and extend our
understanding of this issue. Other
reports in this series address the
effects on mental health, driving,
respiratory and cardiovascular health,
medical use, cognitive function and
edibles. This series is intended for
public health professionals, including
program managers and coordinators,
educators and health promoters,
prevention experts, direct healthcare
providers (e.g., physicians, nurses,
pharmacists), policy and decision
makers, and researchers.
1

Clearing the Smoke on Cannabis: Cannabis Use During Pregnancy and Breastfeeding
2
Background
After alcohol, cannabis (also referred
to as marijuana) is the most widely
used psychoactive substance in
Canada. According to the cross-
sectional National Cannabis Survey,
in 2020, 20.0% of Canadians aged
15 years and older reported using
cannabis in the previous three
months, and 7.9% reported daily
use, a significant increase from 2018
(5.4%) and 2019 (6.1%) (Statistics
Canada, 2021). The use of cannabis
in 2020 was generally more prevalent
among young people (15–24years),
with 19.2% of youth aged 15 to
17years and 35.6% of young adults
aged 18 to 24 years reporting use in
the previous three months.
A growing body of evidence sug-
gests that cannabis use can nega-
tively affect several aspects of people’s lives, including men-
tal and physical health, cognitive functioning, ability to drive
a vehicle, and pre- and postnatal development among chil-
dren. One in a series reviewing the effects of cannabis use
on various aspects of human functioning and development
(Gabrys & Porath, 2019; Konefal et
al., 2019; Renard, 2020), this report
explores the effects of prenatal can-
nabis exposure on offspring, including
the birth outcomes, neurodevelop-
ment processes, behaviour and
mental health of children. Following
a review of the evidence, we discuss
implications for policy and practice.
Much of the available evidence on
this topic comes from three pro-
spective longitudinal cohort studies
and four retrospective cohort stud-
ies. The longitudinal studies describe
the effects of cannabis use during
pregnancy on child development and
behaviour. Table 1 summarizes these
studies’ details. The prospective longi-
tudinal nature of these studies follows
the same group of mothers and chil-
dren over a long period. This allows for
reliable measurement of the extent and timing of cannabis
exposure, as well as many lifestyle variables (e.g., maternal
health, socioeconomic status, maternal use of drugs other
than cannabis) during pregnancy and assesses the develop-
mental differences in children’s behaviour and functioning.
Table 1. Summary of details from three longitudinal, prospective cohort studies evaluating outcomes of maternal cannabis use during pregnancy
Variable
Ottawa Prenatal
Prospective Study (OPPS)
Maternal Health Practices
and Child Development
(MHPCD) Generation R
Reference Fried et al., 1984 Day et. al, 1992 El Marroun et al., 2009
Start year 1978 1982 2001
Location Ottawa, Canada Pittsburgh, USA Rotterdam, Netherlands
Sample demographic Caucasian, predominantly
middle-class families
Mostly black women from low
socioeconomic backgrounds
Multiethnic cohort with
predominantly higher
socioeconomic status
Total sample size 583 763 7,452
Initial sample size (cannabis
exposed
a
during pregnancy)
78 307 214
Categorization of cannabis
exposure
Irregular use (no more than
one marijuana cigarette per
week or 2nd hand smoke),
moderate use (average 2–5
per week) or heavy use
(average use greater than 5
per week)
Light use (between 0.0 and
0.4 average daily joints (ADJ),
moderate use (between 0.4
and 1 ADJ) or heavy use (1 or
more ADJ)
Occasional (monthly),
moderate (weekly), heavy
(daily) or no use
Times at which maternal
cannabis use measured
Rate of use calculated at each
trimester
Rate of use calculated at each
trimester, and at 8 months,
18 months and 36 months
postpartum
Rate of use calculated before
pregnancy, in early pregnancy
and in late pregnancy
a
Including women who also smoked tobacco and who may have only used cannabis during the first trimester.
Cannabis, also called marijuana, refers
to products of the cannabis plant.
It is usually a greenish or brownish
material consisting of the dried
flowering fruiting tops and leaves of
the cannabis plant. Cannabis contains
more than 100 cannabinoids,
with delta-9-tetrahydrocannabinol
(THC) being the main psychoactive
ingredient responsible for the high
that people feel. Cannabidiol (CBD)
is the second-most common
cannabinoid in cannabis. Cannabidiol
is not associated with the high and
is being studied for various medical
applications, such as relieving pain,
anxiety and other chronic conditions.

Clearing the Smoke on Cannabis: Cannabis Use During Pregnancy and Breastfeeding
3
The retrospective studies looked at past and archived data
to examine the potential risk factors (including cannabis
use) that could increase the risk for a disease. Those risks
were compared between participants who were exposed
and not exposed after the exposure and the outcome had
already occurred. Table 2 summarizes the four most rel-
evant retrospective cohort studies describing the effects of
cannabis use during pregnancy on child development and
behaviour. As these studies were conducted before Canada
legalized recreational cannabis occurred in October 2018,
the prevalence of cannabis use may have changed since
then. More data needs to be collected to examine the
effects of legalization on prenatal cannabis use.
Prevalence, Reasons and Perceptions of
Cannabis Use During Pregnancy
In Canada, about 47.6% of women of childbearing age
(i.e., 15–44 years) reported lifetime use of cannabis in 2017
(Statistics Canada, 2019). In 2020, 23% of women aged
16–19 years, 20% of women aged 20–24 years and 19%
of women aged 25 years and older reported daily or almost
daily cannabis use in the past year (Health Canada, 2021c).
Even more striking, in the northern territories of Canada
such as Nunavut, 70% of women aged 15–19 years and
50% of women aged between 25 and 44 years have used
cannabis in the past year (Reece & Hulse, 2020).
The Canadian Alcohol and Drugs Survey (CADS) showed
that in 2019, 5% of women of childbearing age reported
using cannabis during their last pregnancy, and 6% while
breastfeeding (Health Canada, 2021a). Data from the Better
Outcomes Registry & Network (BORN) database of live
and stillbirths in Ontario between April 2012 and December
2017 showed that the prevalence of cannabis use during
pregnancy increased by 61% from 1.2% in 2012 to 1.8%
in 2017 (Corsi, Hsu et al., 2019). Increases in the preva-
lence of cannabis use during pregnancy were predomin-
ately observed among younger women aged 15 to 24
years (5.49%) and those with lower socioeconomic status
(3.11%). Another recent study of 478 pregnant women in
the greater Hamilton area, Ontario, showed that 4.2% of
survey respondents reported using cannabis despite being
aware of potential risks of harm for the fetus (Bartlett et al.,
2020). Another recent survey from a women’s health unit
Table 2. Summary of details from four retrospective cohort studies evaluating outcomes of maternal cannabis use during pregnancy
Retrospective
Cohort Study
ABCD (Winiger &
Hewitt, 2020)
ABCD (Paul et al.,
2020)
BORN (Corsi, Walsh
et al., 2019)
BORN (Corsi et al.,
2020)
Collection of data June 1, 2016, to Oct.
15, 2018, from children
born between 2005
and 2009
June 1, 2016, to Oct.
15, 2018, from children
born between 2005
and 2009
Births and stillbirths
between April 2012
and December 2017
Births occurring
between April 1, 2007,
and March 31, 2012
Location 22 sites in the USA 22 sites in the USA Ontario Ontario
Sample size 11,875 11,489
a
Matched cohort
b
of
98,512 records
Matched cohort
b
of
173,035 records
Cannabis exposed 695 655 (413 were
exposed only before
maternal knowledge
of pregnancy, 235
both before and after
maternal knowledge,
and seven only after
maternal knowledge)
Matched group:
b
5,639 cannabis
exposed
Matched group:
b
2,364 cannabis
exposed
Cannabis exposure Self-reporting ever
using cannabis while
pregnant
Self-reporting using
cannabis either before
maternal knowledge of
pregnancy only, after
maternal knowledge
of pregnancy only
or before and after
maternal knowledge of
pregnancy
Self-reporting ever
using cannabis while
pregnant during
routine prenatal care
Self-reporting ever
using cannabis during
the first prenatal
consultation (occurring
between 11 weeks
2days and 13 weeks
3day of gestation)
Note. ABCD = Adolescent Brain and Cognitive Development cross-sectional studies; BORN = Better Outcomes Registry & Network.
a
Only participants with no missing records of cannabis exposure during pregnancy were included in this study.
b
Matching strategy avoided critical potential confounders and ensured an equal distribution among exposed and nonexposed groups. In those
studies, cohort samples were matched for maternal obstetrical and sociodemographic characteristics between reported cannabis exposed and
nonexposed to reduce disparities in the sample.

Clearing the Smoke on Cannabis: Cannabis Use During Pregnancy and Breastfeeding
4
in Canada showed that 5% of preg-
nant women and 6.3% of breast-
feeding women were using cannabis
regularly (daily or weekly) (Manning
& Drover, 2020). A recent survey on
maternal health of 7,111 women in
Canada has shown that 3.1% of
respondents reported using can-
nabis during pregnancy and 2.6%
while breastfeeding (Grywacheski
et al., 2021). Sociodemographic
and mental health factors, including
lower level of education, thoughts of
self-harm, postpartum depression,
anxiety symptoms or any combina-
tion of these were associated with
cannabis use during pregnancy,
breastfeeding or both. Finally, a
study conducted in British Columbia
showed that maternal cannabis use
has increased over the past decade
from 2.2% in 2008 to 3.3% in 2016
(Luke et al., 2019). Younger age,
polysubstance use, lower socio-
economic status and history of men-
tal illness were factors associated
with cannabis use during pregnancy.
Overall, the prevalence of cannabis use during pregnancy
in several Canadian studies ranges from about 2% to 5%
(Badowski & Smith, 2020). However, because prevalence
measures largely rely on self-reporting, prevalence rates are
likely underestimated due to stigma or other fears (i.e., child
services intervention). For example, a study conducted in
Pittsburgh found that only 36% of pregnant patients who
tested positive for etrahydrocannabinol (THC) had disclosed
their cannabis use (Chang et al., 2017). An older study ana-
lyzing the effects of prenatal cannabis and alcohol exposure
on child academic performance at age 10 showed that 14%
of women were using cannabis regularly (i.e., smoking one
or more joints daily) during the first trimester of pregnancy,
compared with 5.3% and 5.0% during second and third tri-
mesters, respectively (Goldschmidt et al., 2012). Prevalence
of cannabis use during pregnancy can be as high as 15% to
28% in disadvantaged, urban or low-income women (Beatty
et al., 2012; Passey et al., 2014; Schempf & Strobino, 2008).
Other recent studies have indicated that in the United States,
younger age (before 25 years), lower education level, lower
socioeconomic status (unemployment, lower income), being
non-Hispanic or African-American, earlier trimester of preg-
nancy, marital status (i.e., not married), poor mental health
(i.e., anxiety or depression) and con-
comitant use of tobacco, alcohol or
both were risk factors for cannabis use
among pregnant women (Bayrampour
et al., 2019; Corsi, Hsu, et al., 2019;
Odom et al., 2020).
In addition, with easier accessibility to
cannabis, more legal product choices
available and increasing social accept-
ance, the prevalence of cannabis use
may have increased since the legaliza-
tion of nonmedical cannabis in October
2018 in Canada. For example, canna-
bis use during pregnancy (confirmed
by urine toxicology test) increased in
California after legalization from 6%
to 11% (Lee et al., 2020). Another
study showed that the prevalence of
cannabis use during pregnancy (con-
firmed by urine toxicology test) was
as high as 18% in Colorado, which
also legalized recreational cannabis
(Rodriguez et al., 2019). In Ontario,
Canada, a prospective longitudinal
cohort study examined the conse-
quences of nonmedical cannabis legalization a year follow-
ing legalization (Turna et al., 2021). It showed that cannabis
use decreased among adults who were using cannabis
before legalization and increased among adults who were
not using cannabis before legalization.
While the impact of legalization on cannabis use in Canada
is not well established and more data need to be collected,
the prevalence of cannabis use may have changed since
the studies conducted before legalization.
Reasons for Cannabis Use During
Pregnancy
Over the past years, there has been an increasing belief that
cannabis is harmless and can relieve some of the symp-
toms of pregnancy, such as morning sickness, nausea and
vomiting, anxiety, and sleep disorders. This belief can be
promoted by healthcare providers, the cannabis industry
and nonmedical employees at retail cannabis dispensaries
(Bayrampour et al., 2019; Dickson et al., 2018; Metz &
Borgelt, 2018). For example, 69% of pregnant women in
Colorado cannabis dispensaries were recommended can-
nabis to alleviate morning sickness (Dickson et al., 2018).
It is also common for pregnant women to seek information
about cannabis and pregnancy from family and friends, as
There are different ways to use
cannabis. Cannabis can be ingested
(edible cannabis, oils, drinks, pills),
inhaled (smoked or vaped) or applied
to the skin. The duration of cannabis’s
effects depends on how it is used.
When inhaled, cannabis intoxicating
effects start within a few seconds to
a few minutes and peak within 30
minutes. Effects can last up to six
hours and residual effects can last up
to 24 hours. When ingested, cannabis
intoxicating effects do not kick in for
about 30 minutes to two hours and
peak at about four hours. The effects
can last up to 12 hours after use and
residual effects can last up to 24
hours. This timing differs from smoking
or vaping cannabis, where the effects
start to be felt within a few seconds or
minutes and peak at about 30 minutes.

Clearing the Smoke on Cannabis: Cannabis Use During Pregnancy and Breastfeeding
5
well as the internet and social media. However, a great deal
of inaccurate information is circulating on untrusted online
sources about the potential positive effects of cannabis on
some of these pregnancy symptoms. As a consequence,
many pregnant women report using cannabis during preg-
nancy to alleviate morning sickness, pain and mood disor-
ders (Metz & Borgelt, 2018). In another survey conducted in
Colorado, 63% of women reported using cannabis during
pregnancy to alleviate anxiety and depression symptoms,
and 60% reported using it for pain relief (Committee on
Obstetric Practice, 2017). Similarly, in a Canadian women’s
health unit survey, among the 5% of pregnant women using
cannabis, relieving anxiety symptoms (33.3%), sleep dis-
turbances (22.2%) and nausea or vomiting (22.2%) were
the most common reasons reported for cannabis use
(Manning & Drover, 2020).
Despite these findings, there is no evidence showing
that cannabis use during pregnancy can alleviate these
symptoms. Further robust randomized controlled studies
examining the efficacy of cannabis in alleviating symptoms
associated with pregnancy as well as its safety during preg-
nancy are still needed. Meanwhile, increasing awareness
about the potential risks of cannabis use during pregnancy
and breastfeeding remains essential.
Perceptions of Cannabis Use During
Pregnancy
Pregnant women who use cannabis generally perceive
cannabis as having low risks for the fetus, compared with
pregnant women who do not use cannabis (Weisbeck et
al., 2021). A survey of 306 women in the United States
showed that 35% of pregnant women were using canna-
bis. Among those, 34% were not willing to quit cannabis
use during their pregnancy. Three-quarters (75%) of preg-
nant women who were using cannabis were more likely to
perceive cannabis use as harmless, compared with preg-
nant women who quit cannabis use (Mark et al., 2017).
In the 2021 Canadian Cannabis Survey, 83% of those who
used cannabis did not agree that it was reasonable to use
cannabis while pregnant or breastfeeding, which was the
same as in 2020 (Health Canada, 2021b). That is com-
pared with 88% of those who did not use cannabis in the
previous 12 months, which was down slightly from 90%
in 2020. In addition, 95% of women aged 16 to 50 years
who had given birth in the previous five years reported not
having used cannabis once they knew they were pregnant,
which was unchanged from 2020. Finally, 92% of women
reported not having used cannabis while breastfeeding
their child, which was also unchanged.
Another recent survey from the greater Hamilton area in
Ontario showed that most of the women surveyed were aware
that cannabis can pass to the fetus through the placenta
(94.3%) or to the infant through breastmilk (91.2%) (Bartlett
et al., 2020). Both can have risks to the infant’s development.
However, despite this high proportion of aware women, 4.2%
of them were still using cannabis while pregnant.
In a recent Canadian women’s health unit survey, 22.6% of
respondents said they believed that cannabis use during
pregnancy and breastfeeding was harmless, while 30.4%
were unsure of the potential harm of cannabis use during
pregnancy and breastfeeding (Manning & Drover, 2020).
In the United States, a qualitative study examining attitudes
and beliefs about prenatal cannabis use showed that preg-
nant women who used cannabis during pregnancy had
conflicting attitudes about their cannabis use while pregnant
(Chang et al., 2019). They reported trying to reduce can-
nabis use during pregnancy because of the potential risks
for the developing baby. On the other hand, they perceived
cannabis as being safer than other substances, including
prescribed medications, because it is a natural plant.
Finally, an integrative review that analyzed women’s percep-
tion showed that women who use cannabis during preg-
nancy generally perceived cannabis use as harmless com-
pared with women who do not use cannabis (Bayrampour
et al., 2019). Most pregnant women reported a lack of
information or recommendations from and communication
with their healthcare providers about the health effects of
prenatal cannabis use. This reinforces the idea that canna-
bis use during pregnancy may be harmless or insignificant.
All these findings have implications for how healthcare pro-
viders discuss the use of cannabis with pregnant patients.
Informed discussions with healthcare providers about the
potential adverse effects of using cannabis during pregnancy
are needed to help women make informed and healthy
choices (Bayrampour et al., 2019). In addition, person-
centred, harm reduction and trauma-informed approaches
are needed during these discussions to help ensure informed
and nonjudgmental discussions and build a trusting relation-
ship between healthcare providers and pregnant patients.
Effects on Pregnancy, Fetal Development
and Birth Outcomes
Fetal Development and Neonatal Birth
Outcomes
After controlling for maternal tobacco, alcohol and illicit
drug use and various demographic covariates, there is
conflicting evidence of an association between cannabis

Clearing the Smoke on Cannabis: Cannabis Use During Pregnancy and Breastfeeding
6
use during pregnancy and an increased risk of pregnancy
complications, premature birth, small head circumfer-
ence, small length, stillbirth or major congenital abnormal-
ities (Gunn et al., 2016; Metz & Stickrath, 2015; National
Academies of Sciences, Engineering, and Medicine, 2017).
However, substantial evidence highlights an elevated risk
for low birth weight in infants from mothers who used can-
nabis during pregnancy (National Academies of Sciences,
Engineering, and Medicine, 2017). Further, while reports
on the effects of prenatal cannabis exposure are mixed,
heavy cannabis use is more strongly associated with cer-
tain adverse outcomes of pregnancy.
In the Generation R study, maternal cannabis use dur-
ing pregnancy was associated with reduced fetal growth
in mid and late pregnancy as well as a lower birth weight
(El Marroun et al., 2009). These associations were
independent of various lifestyle and socioeconomic factors.
The results from this study also suggested a dose–response
relationship such that heavier cannabis use during preg-
nancy was particularly associated with lower birth weight.
Findings from the Maternal Health Practices and Child
Development (MHPCD) study noted a small but significant
negative relationship between cannabis use during the first
trimester and length of the child at birth (Day et al., 1991).
In a study of a large cohort of Australian women presenting
for public prenatal care at a large hospital between 2000
and 2006, Hayatbakhsh et al. (2012) reported that use of
cannabis during pregnancy significantly predicted negative
birth outcomes, including low birth weight, preterm birth,
small for gestational age and admission to the neonatal
intensive care unit. These effects were independent of
the mother’s sociodemographic characteristics, cigarette
smoking, alcohol consumption and use of illicit drugs.
In contrast, the Ottawa Prenatal Prospective Study (OPPS)
did not observe any differences in growth measures at birth
between infants born to women using cannabis and those
not using cannabis (Fried & O’Connell, 1987). Fried et al.
(1984) noted a statistically significant reduction of about
one week in the gestational age of infants born to moth-
ers in the OPPS who used cannabis six or more times per
week compared with those who did not.
Two recent meta-analyses assessed neonatal health out-
comes following maternal cannabis exposure. The first
included results from 24 studies that did not control for poly-
substance use and found that exposure to cannabis in utero
was associated with decreased birth weight and an increased
likelihood of admission to the neonatal intensive care unit
(Gunn et al., 2016). The second included results from 31
observational cohort or case-control studies where canna-
bis and other substance use had been recorded (Conner et
al., 2016). The authors noted a significantly elevated risk of
low birth weight and premature birth in women who used
cannabis. That risk doubled when the frequency of cannabis
use was at least once per week. However, these associations
disappeared after adjusting for tobacco use.
Three retrospective cohort studies not included in these
meta-analyses adjusted for concurrent tobacco use and
reported mixed results on risks associated with prenatal
cannabis exposure (Chabarria et al., 2016; Ko et al., 2018;
Warshak et al., 2015). Chabarria et al. (2016) found that
while smoking only cannabis had no significant effect on
any of the birth outcomes assessed, both cannabis and
tobacco were associated with an increased risk for low birth
weight, preterm birth and decreased head circumference.
Ko et al. (2018) only looked at mean infant birth weight and
gestational age. After controlling for relevant covariates,
such as cigarette smoking, they found no significant dif-
ferences in infants from women who used cannabis during
pregnancy. Warshak etal. (2015) reported an increased risk
for admission to the neonatal intensive care unit and small
for gestational age but no effect on birth weight. Smoking
cannabis during pregnancy was also found to increase the
odds of having an infant with low birth weight by almost
three times, although authors did not adjust their analysis
for tobacco or alcohol use (Campbell et al., 2018)
The large Ontario retrospective cohort study using the birth
registry (BORN) examined the association between pre-
natal cannabis exposure and adverse maternal and peri-
natal outcomes (Corsi, Walsh, et al., 2019). Authors ana-
lyzed births and stillbirths among women aged 15 years
and older between April 2012 and December 2017. They
found that in women who reported cannabis use during
pregnancy (1.4%), cannabis exposure was significantly
associated with increased frequency of small for gesta-
tional age, placental abruption, greater transfer to neonatal
intensive care and an abnormal five-minute Apgar score
1
of
less than four.
In another recent study, cannabis use during pregnancy
(among other substances use) was associated with an
increased risk of small for gestational age (47% increased),
preterm birth (27% increased) and intrapartum stillbirth
(184% increased) (Luke et al., 2019). However, caution
should be taken as the authors did not rule out the effects
that other substance use may have had on pregnancy
outcomes.
1
The five-minute Apgar test is performed five minutes after birth on the newborn by the healthcare provider to examine different parameters such as
breathing, skin color, heart rate, muscle tone and reflexes. The score indicates to the healthcare provider how the newborn is doing outside of the womb.

Clearing the Smoke on Cannabis: Cannabis Use During Pregnancy and Breastfeeding
7
Finally, a retrospective observational cohort study was
conducted using health records data from 3,435 women
who received prenatal care and a subsequent singleton
live birth in Minnesota. Among those women, 283 (8.2%)
tested positive for THC via urine toxicology assays. Authors
showed that exposure to cannabis during pregnancy was
associated with small for gestational age and increased
abnormal 12-month developmental screens (Kharbanda et
al., 2020). Similarly, increased risk of small for gestational
age was shown in another recent study in which prenatal
THC exposure was also confirmed using urine analyses
(Rodriguez et al., 2019).
In these studies, the authors concluded that the discrep-
ancy in other findings evaluating the effects of prenatal
exposure may be due to the uncertainty or underestima-
tion of prenatal cannabis use. In support of this idea, a
recent study showed that self-reported cannabis use dur-
ing pregnancy (confirmed by urine toxicology testing) was
associated with adverse outcomes, including preterm birth,
hypertensive disorders of pregnancy,
stillbirth or small for gestational age
(Rodriguez et al., 2019). Importantly,
the odds of adverse outcomes were
higher in women who had more than
one positive THC urine test com-
pared with women who had negative
THC tests. Using THC urine analyses
to better confirm the use of cannabis
during pregnancy would help to bet-
ter estimate the effects of cannabis
use during pregnancy.
Despite difficulties determining the
unique effects of cannabis exposure
on pregnancy and fetal development,
the National Academies of Sciences,
Engineering, and Medicine (2017)
report concluded that there was sub-
stantial evidence for a statistically sig-
nificant association between maternal cannabis smoking
and low birth weight of infants exposed in utero. Low birth
weights were subsequently associated with poor long-term
outcomes throughout childhood and adulthood, including
increased risk for Type 2 diabetes, hypertension, cardio-
vascular disease and respiratory problems (Gluckman
etal., 2008; Statistics Canada, 2016).
However, it is yet unknown whether smoking as a means
of use can have negative effects rather than cannabis itself.
Cannabis smoking has been and still is the most common
method of cannabis use. Therefore, some of the negative
outcomes for infants of mothers using cannabis may be in
part related to other toxic chemicals inhaled when smoking.
To date, there have been no studies that have examined if
different methods of cannabis use (smoking, vaping, sub-
lingual or ingested) have different effects on fetal outcomes.
Further studies are needed to explore this question.
Congenital Abnormalities
Only a few correlational studies have demonstrated a link
between congenital abnormalities and prenatal cannabis
use. For instance, after adjusting for socioeconomic vari-
ables and the use of other substances such as tobacco
and opioids, a recent study analyzing health record data
in Canada found a positive correlation between rates of
cannabis use and rates of congenital anomalies in the terri-
tories (Reece & Hulse, 2020). This included cardiovascular
defects, orofacial clefts, Down syndrome and gastroschisis
(a defect in an infant’s abdominal wall). However, this find-
ing should be treated with caution as this is a geospatial
paper and many confounding factors were not considered.
Other studies have also shown poten-
tial associations between prenatal
cannabis use and congenital anom-
alies, such as ventricular septal defects
(Williams et al., 2004), bowel matting
(Weinsheimer et al., 2008), gastro-
schisis, anencephaly and esophageal
atresia (van Gelder et al., 2014).
Findings from the above-mentioned
studies should be interpreted with
caution because a “positive correla-
tion” does not mean a “causal asso-
ciation” between prenatal cannabis
use and offspring congenital anom-
alies. Confounding factors may have
a role in this relationship, which may
establish causality between prenatal
cannabis exposure and congenital
anomalies. Most of the available studies examining this rela-
tionship, including the prospective longitudinal birth cohorts,
have not found an association between prenatal cannabis
use and increased risk for congenital anomalies in children
(Kharbanda et al., 2020).
Effects on Neurocognitive Functioning
and Neurodevelopmental Processes
Neurocognitive Functioning
Findings from the OPPS and MHPCD longitudinal stud-
ies suggest that maternal cannabis use during pregnancy
Regular and Heavy Cannabis Use
There is no single definition in the
scientific literature of what constitutes
regular cannabis use. The phrase
generally refers to weekly or more
frequent use over months or years
and poses a risk for adverse health
effects. Terms that are often used
interchangeably with regular use
include frequent use, chronic use and
long-term use. By contrast, heavy use
typically refers to daily or more frequent
use and can be a sign of dependence
and cannabis use disorder.

Clearing the Smoke on Cannabis: Cannabis Use During Pregnancy and Breastfeeding
8
18 months 3–6 years 9–11 years 14–16 years
17–22 years
Increased aggressive
behaviour
c
Attention deficits
(females)
c
Deficits in verbal and
perceptual skills,
a,b
verbal, quantitative
and visual reasoning,
a,b
short-term memory,
a,b
attention
a,b
and
vigilance
b
Hyperactivity
a,b
Impulsivity
a,b
Deficits in abstract
and visual reasoning,
a,b
attention,
b,d
executive
functioning,
a,b
reading,
a,b
spelling,
a,b
attention,
b,d
and internalizing,
externalizing, and social
behaviours
d
Hyperactivity
a,b
Impulsivity
b
Depressive and anxious
symptoms
b
Psychotic-like
experiences
d
Thoughts disturbances
d
Long-term sleep
disorders
e
Deficits in visual-
cognitive functioning,
a
academic
achievement,
b
information processing
speed
b
and visual-
motor co-ordination
b
Delinquency
b
Deficits in executive
functioning,
a
response
inhibition
a
and
visuospatial working
memory
a
Smoking
a,b
Substance use
a,b
Early initiation of
substance use
a,b
a
Ottawa Prenatal Prospective Study (Fried et al., 1984)
b
Maternal Health Practices and Child Development (Day et al., 1992)
c
Generation R (El Marroun et al., 2009)
d
Adolescent Brain and Cognitive Development (Paul et al., 2021)
e
Adolescent Brain and Cognitive Development (Winiger & Hewitt, 2020)
Figure 1. Neurocognitive and Behavioural Effects
affects children’s neurocognitive development. Beginning at
age three to four years, children of mothers who used can-
nabis heavily while pregnant have shown deficits in mem-
ory, verbal and perceptual skills, and verbal and visual rea-
soning after adjusting for potentially confounding variables
2
(Day etal., 1994; Fried & Watkinson, 1990). In contrast, the
results from the Generation R study did not find evidence of
such cannabis-related deficits when children were assessed
at about three years old (El Marroun, 2010). Impaired verbal
and quantitative reasoning and short-term memory have
also been found in the MHPCD among six-year-old chil-
dren whose mothers reported smoking one or more can-
nabis cigarettes per day while pregnant (Goldschmidt et al.,
2008). Both the OPPS and MHPCD studies reported that in
children about nine years of age, prenatal cannabis expos-
ure was linked with impaired abstract and visual reasoning,
poor executive functioning (i.e., visual-motor integration,
nonverbal concept formation and problem-solving) and
deficits in reading, spelling and academic achievement
(Fried et al., 1998; Fried & Watkinson, 2000; Goldschmidt
et al., 2004; Richardson et al., 2002). Vulnerability in visual-
cognitive functioning has been shown to persist into early
adolescence among those children heavily exposed to
cannabis in utero (Fried et al., 2003).
Prenatal exposure to heavy maternal cannabis use during
the first trimester also predicted significantly poorer scores
on academic achievement tests (particularly in reading) at
the age of 14 years in the MHPCD (Goldschmidt et al.,
2012). Interestingly, these latter effects were found to be
related to prenatal cannabis exposure on intelligence test
performance at age six years, attention problems and
2
In all three longitudinal studies, the analyses controlled for various covariates such as the children’s gender and ethnicity, home environment,
maternal socioeconomic status, prenatal exposure to tobacco and alcohol, and current maternal substance use.

Clearing the Smoke on Cannabis: Cannabis Use During Pregnancy and Breastfeeding
9
depression symptoms at age 10 years and early start of
cannabis use. At the age of 16 years, deficits in informa-
tion processing speed, interhemispheric transfer of infor-
mation and visual-motor coordination have been linked
with prenatal exposure to cannabis (Willford et al., 2010)
These effects were found with light to moderate prenatal
cannabis exposure in the MHPCD. However, general intelli-
gence does not appear to be affected by prenatal cannabis
exposure (Fried et al., 1998; Fried et al., 2003).
Findings from brain imaging studies of young adults aged
18–22 years enrolled in the OPPS showed that in utero
cannabis exposure negatively affects the neural circuitry
involved in aspects of executive functioning, including
response inhibition, attention and visuospatial working
memory (Smith et al., 2004; Smith et al., 2006; Smith et
al., 2016). Consistent with these findings, results from a
neuroimaging study with the Generation R cohort showed
altered brain morphology, specifically in the frontal cortex,
in children aged 6–8 years who were exposed prenatally
to cannabis (El Marroun etal., 2016). These findings are
also consistent with a report of altered functional connec-
tivity in neonates with prenatal cannabis exposure and
are particularly noteworthy as they show that smoking
cannabis during pregnancy can lead to long-term chan-
ges in children’s neurocognitive development (Grewen
et al., 2015).
In all three longitudinal studies mentioned above, the analy-
ses controlled for various covariates, such as the children’s
gender and ethnicity, home environment, maternal socio-
economic status, prenatal exposure to tobacco and alco-
hol, and current maternal substance use.
Finally, the longitudinal Adolescent Brain and Cognitive
Development (ABCD) study recruited children ages 9 to 11
years across the United States (Paul et al., 2021). Children
in this study will be followed until age 20 years and will
help characterize normal adolescent brain development
and factors that can affect neurodevelopment. One of the
ABCD cross-sectional studies examined whether prenatal
cannabis exposure in 655 children exposed to cannabis
prenatally before and after being aware of the pregnancy
can be associated with psychopathology symptoms in
middle childhood, such as psychotic-like experiences,
internalizing or externalizing problems, attention deficits,
thought disturbances and social behaviour problems (Paul
et al., 2021). Cognition, sleep, birth weight, gestational age
at birth, body mass index and brain structure (i.e., total
intracranial volume, white matter volume and grey matter
volume) were also analyzed. The researchers accounted
for multiple confounding factors that were included in the
ABCD cross-sectional studies. They included ethnicity (e.g.,
White, Black, Asian, Indigenous, Pacific Islander, Hispanic
and other), first-degree familial history of psychopathology
(e.g., depression, psychosis, anxiety, mania and antisocial
behaviour), marital status, prenatal exposure to tobacco or
alcohol, unplanned pregnancy, prenatal vitamin, alcohol or
tobacco use, child sex, twin or multiple pregnancy, house-
hold income, birth weight, maternal age at birth, gestational
age when pregnancy was discovered, child age and moth-
er’s education. Findings from this ABCD cross-sectional
study showed that prenatal cannabis exposure after being
aware of the pregnancy was associated with greater dis-
turbances in attention, thought and social behaviours (Paul
et al., 2021).
Conversely, a recent critical review of data from 45 longi-
tudinal studies, including data from OPPS and MHPCD
cohorts, investigated the effects of prenatal cannabis
exposure on cognitive functioning in individuals aged
from 0 to 22 years (Torres et al., 2020). The authors
concluded that there were relatively few cognitive defi-
cits observed in children who were prenatally exposed
to cannabis. According to the authors, most studies that
have shown cognitive deficits did not compare measures
against a normative database that would have confirmed
that findings were statistically significant. Normative data
help characterize what is “normal” in a large, random and
representative population at a specific period and include
important other factors, such as age and education,
for example.
Neurodevelopmental Outcomes
A large Canadian retrospective cohort study using the
birth registry (BORN) from Ontario, analyzed the relation-
ship between cannabis use during pregnancy and neuro-
developmental outcomes in childhood (Corsi et al., 2020).
The authors analyzed births occurring between April 1,
2007, and March 31, 2012. Their findings showed that
prenatally cannabis exposed children had a 50% increased
risk for an autism diagnosis even after controlling for con-
founding factors, such as income, preterm birth and the
use of other substances (Corsi et al., 2020). However,
these findings should be taken with caution as other resid-
ual confounding factors, such as genetic vulnerabilities,
environmental factors, fetal and postnatal environment,
and dose and type of cannabis used, might still play a
role in this relationship, which ascertain causality between
prenatal cannabis exposure and the onset of later child-
hood neurodevelopmental disorders (Corsi et al., 2020).
The authors also pinpointed a small increased risk (11% to
22%) for developing intellectual deficits, learning disorders

Clearing the Smoke on Cannabis: Cannabis Use During Pregnancy and Breastfeeding
10
and ADHD in prenatally cannabis exposed children com-
pared with nonprenatally exposed children. However, these
associations were no longer observed after controlling for
confounding factors (Corsi et al., 2020).
Behavioural Effects
Behavioural and Emotional Functioning
Outcomes
The behavioural effects of prenatal cannabis exposure have
also been documented, although it is unclear as to how
early such effects first present themselves. The Generation
R study has reported that prenatal exposure to cannabis
is associated with an increased risk of aggressive behav-
iour and attention problems as early as 18 months of age
in girls, but not boys (El Marroun et al., 2011). At the age
of four years, the OPPS failed to find evidence of a nega-
tive relationship between cannabis exposure and attention
(Fried & Watkinson, 1990), whereas the MHPCD found
impaired vigilance among exposed children at this age
(Noland et al., 2005). When children reached age six years,
the effects of maternal cannabis use during pregnancy
become much more evident. Children who were prenatally
exposed to cannabis— particularly those who were heavily
exposed — were found to be more hyperactive, inatten-
tive and impulsive compared with children who were not
exposed prenatally to cannabis (Fried et al., 1992; Leech
et al., 1999). At age 10 years, prenatally exposed children
display increased hyperactivity, inattention and impulsivity,
and show increased rates of delinquency and externaliz-
ing problems as reported by their mothers and teachers,
compared with children who were not exposed prenatally
to cannabis (Fried et al., 1998; Goldschmidt et al., 2000;
Richardson et al., 2002). The MHPCD reported that chil-
dren who were heavily exposed to cannabis during the
first trimester (i.e., one or more joints per day) were almost
twice as likely to display delinquent behaviour at the age
of 14 years as the children who were not exposed to can-
nabis or those who were exposed to lesser amounts (Day
et al., 2011). The authors also noted that the relationship
between prenatal exposure to cannabis and delinquent
behaviour appeared to be mediated by the effects of can-
nabis on depressive symptoms and by attention deficits in
children exposed to cannabis. However, in children ages
13–16 years, the effects of prenatal cannabis exposure
on some aspects of attention (i.e., flexibility, encoding and
focusing) appeared to wane (Fried et al., 2003).
Similarly, another study assessed the potential causal asso-
ciation between prenatal cannabis exposure and behav-
ioural or emotional functioning in Dutch children aged seven
to 10 years (El Marroun et al., 2019). Findings showed that
maternal cannabis use during pregnancy was associated
with child externalizing behaviour problems, including harm-
ful, aggressive or antisocial behaviours directed at others
such as physical or relational aggression, delinquency,
bullying, defiance and vandalism. However, both maternal
cannabis use before pregnancy and paternal cannabis use
were also associated with externalizing problems in children.
This suggests that the association between prenatal can-
nabis exposure and behavioural or emotional functioning
problems observed in children was not caused by direct
in utero cannabis effects on fetal development but rather
through residual confounding variables, such as shared
genetic vulnerabilities, environmental factors, other variables
such as parental behaviours, or any combination of these
(El Marroun et al., 2019).
Consistent with this idea, a study showed that both pre-
natal tobacco and cannabis exposure were indirectly asso-
ciated with child externalizing problems at 16 months of
age, an effect potentially due to “harsh” parenting during
caregiver–child interactions (Schuetze et al., 2019). These
findings support other studies showing that regulation and
externalizing behaviour problems in children may be asso-
ciated with “harsh” parental behaviours, such as insensitiv-
ity, anger or hostility (Bradley & Corwyn, 2007; Gartstein
et al., 2013; Kochanska & Knaack, 2003; Velders et al.,
2011), behaviours that can be associated with cannabis
use (Ansell et al., 2015). Therefore, these data suggest
that beyond the potential direct effects of cannabis on fetal
development, regular use of cannabis by one or both par-
ents and associated parenting behaviours can also contrib-
ute to transgenerational behavioural or emotional problems.
Sleep Patterns
The long-term effects of prenatal cannabis exposure
on child sleep patterns were analyzed in another ABCD
cross-sectional study (Winiger & Hewitt, 2020). After con-
trolling for various confounding variables, the authors found
that maternal prenatal cannabis exposure was associated
with long-term sleep disorders, such as difficulty initiating
and maintaining sleep, arousal disorders, irregular sleep–
wake disorders and excessive drowsiness in children aged
9–10 years (Winiger & Hewitt, 2020).
These findings were consistent with another older study
showing that prenatal maternal cannabis exposure was
associated with long-term nocturnal sleep disturbances in
children aged three years (Dahl et al., 1995), suggesting
that in utero exposure to cannabis may have long-term
negative effects on children’s circadian regulation. Again,
other residual confounding variables, such as shared
genetic vulnerabilities, environmental factors or other

Clearing the Smoke on Cannabis: Cannabis Use During Pregnancy and Breastfeeding
11
variables, such as parental behaviours, can also play a
role in this relationship.
Substance Use
There is also accumulating evidence that shows prenatal
cannabis exposure may contribute to the start and fre-
quency of substance use during adolescence. Animal
studies showed that repeated exposure to THC in early
development may enhance responses to other addict-
ive substances later in life (Cadoni et al., 2001; Panlilio
etal., 2013). Porath and Fried (2005) reported that 16- to
21-year-old children (particularly males) of women who
used cannabis during pregnancy were at increased risk,
in a dose-related manner, for starting and the daily use of
tobacco and cannabis, compared with children of mothers
who did not use cannabis during pregnancy. Similar results
were noted by Day et al. (2006). At age 14 years, children of
mothers who used cannabis heavily while pregnant not only
reported using this substance more frequently than children
of women who did not use it, but they also started using
it at an earlier age. These findings were also evident when
the offspring were 22 years of age (Sonon et al., 2015).
The likelihood of cannabis use was related to the extent of
prenatal exposure.
The long-term behavioural effects of maternal cannabis
exposure may be particularly relevant in populations where
other socioeconomic risk factors are also present. The
continued use of cannabis by one or both parents in addi-
tion to parental attitudes toward cannabis can contribute to
transgenerational trends in substance use.
Effects on Children’s Mental Health
Depressive and Anxious Symptoms
Some evidence shows that in utero cannabis exposure can
be associated with symptoms of depression and anxiety.
After controlling for other drug use during pregnancy and
risk factors for childhood depression, children of women
using cannabis during pregnancy had significantly more
depressive and anxious symptoms at age 10 years com-
pared with children of women who did not use cannabis
during pregnancy (Gray et al., 2005; Leech et al., 2006).
However, genetic and epigenetic mechanisms
3
can also
contribute to an increased risk of psychiatric disorders,
including anxiety and depression. For example, abnormal-
ities in dopaminergic activity have been shown in humans
exposed to cannabis in utero. The effect is believed to be
mediated through epigenetic mechanisms in brain areas
involved in anxiety and depression, such as the amyg-
dala, nucleus accumbens and ventral striatum (DiNieri
et al., 2011; Wang et al., 2004). Dopaminergic activity
abnormalities are important neurobiological markers of
psychiatric diseases, such as schizophrenia, anxiety and
depression disorders.
A recent study has shown that maternal cannabis use was
associated with increased anxiety, aggression and hyper-
activity in early childhood (i.e., ages 3 to 6 years) as well as
with the stress hormone, cortisol (Rompala et al., 2021).
This behavioural phenotype was associated with decreased
placental expression of important genes involved in immune
function, including proinflammatory cytokines and immune
cell–type markers. More studies are needed to better
understand the relationships between maternal cannabis
use, immune function and anxiety phenotype in children.
Psychotic Symptoms
There is also some evidence that shows that prenatal can-
nabis exposure is associated with psychotic symptoms.
For instance, data from the MHPCD study showed that
young adults who were exposed prenatally to cannabis
were 1.3 times more likely to display psychotic symptoms
compared with unexposed young adults after controlling
for other significant covariates (Day et al., 2015).
Consistent with these findings, a recent prospective
cohort study analyzing data from the Generation R cohort
examined the potential link between parental (maternal
and paternal) cannabis use during pregnancy and the
onset of childhood psychotic symptoms (Bolhuis et al.,
2018). They found that both maternal and paternal can-
nabis use were associated with greater psychotic-like
symptoms in children aged 10 years. They suggested
the existence of other etiologic factors, such as genetics,
environment or familial behaviours, rather than direct in
utero mechanisms that may be involved in the relation-
ship between parental cannabis use and the onset of
psychotic experiences in children.
More recently, findings from the ABCD cross-sectional
study showed that prenatal cannabis exposure after being
aware of pregnancy was associated with greater psycho-
pathology symptoms at ages nine to 11 years even after
accounting for potentially confounding variables (Paul et
al., 2021). The authors suggested that prenatal canna-
bis exposure may be associated with an increased risk of
psychopathological symptoms, including psychotic-like
experiences, and cognitive and social disturbances, in
3
Epigenetic modificationsare alterations in the expression of a gene and involve complex molecular mechanisms, such as DNA methylation and histone
modification. Environmental factors, such as diet, stress, pollution, toxicants, substance use and inflammation, can play important roles in epigenetic
modifications. Epigenetic modifications can lead to diseases, including cancers, autoimmune disorders, psychiatric diseases and diabetes.

Clearing the Smoke on Cannabis: Cannabis Use During Pregnancy and Breastfeeding
12
middle childhood and concluded
that pregnant women should avoid
using cannabis.
The potential impact of prenatal
cannabis exposure on the mental
health of children is critical to their
long-term health and well-being and
needs to be examined more care-
fully in further longitudinal studies.
Breastfeeding
Breastfeeding provides many health
benefits to the development of an
infant, but these benefits must be
weighed against any potential risks
resulting from exposure to can-
nabis during lactation. Concerns
about the use of cannabis during
lactation stem from observations
in humans showing that THC is
secreted in breastmilk (de Oliveira
Silveira et al., 2017; Garry et al.,
2009; Marchei et al., 2011; Merritt
et al., 2016; Metz & Stickrath, 2015)
and is also absorbed, metabolized
and excreted by the infant (Djulus et
al., 2005; Garry et al., 2009; Liston,
1998; Perez-Reyes & Wall, 1982).
In addition to THC, cannabidiol
(CBD) can also be found and can
accumulate in breastmilk after
maternal cannabis inhalation or
edible ingestion (Moss et al., 2021).
This is because cannabinoids are
highly lipophilic compounds and
can be stored in breastmilk, which
is a rich source of healthy fats.
Cannabinoid levels found in breastmilk mostly depend on
the dose and frequency of maternal cannabis use.
One study estimated that within four hours after a single
inhalation of cannabis, breastfed infants ingest about 2.5%
(range from 0.4% to 8.7%) of the maternal dose of THC
(Baker et al., 2018). Another older analysis calculated an
infant’s exposure to THC through ingestion in one feeding
to be 0.8% of the mother’s consumption (Bennett, 1996).
Other studies have shown that THC levels can stay in
breastmilk from six days to six weeks following maternal
cannabis use, with a THC half-life estimation of 20 days
(Bertrand et al., 2018; Cannabis, 2021). A prospective,
observational pharmacokinetic
study estimated the amount and
duration of THC levels in breast-
milk of 25 women who used can-
nabis while pregnant and gave birth
between Nov.1, 2016, and June 30,
2019 (Wymore et al., 2021). Data
showed that, among seven women
who self-reported abstinence from
cannabis (which was confirmed
by plasma analysis), the estimated
half-life of THC in breastmilk was
17 days, with an estimated elimin-
ation time greater than six weeks.
Therefore, the idea of “pumping
and dumping” breastmilk right after
maternal cannabis use to reduce
infant cannabis exposure during
breastfeeding does not seem to be
relevant.
The effects of maternal canna-
bis exposure on infants through
breastmilk are not well studied. The
potential long-term effects of such
exposure on an infant’s developing
brain are still poorly documented
and any conclusions are generally
confounded by in utero cannabis
exposure. Several reports suggest
that the use of cannabis during
breastfeeding contributes to nega-
tive short-term effects on infants,
including sedation, lethargy and
poor feeding habits (Djulus et al.,
2005; Liston, 1998; Miller, 2012).
Two limited studies with very small
sample sizes have attempted to
examine the isolated effects of can-
nabis exposure through breastmilk on long-term infant
health and development. The first study reported that
occasional use of cannabis during lactation did not affect
motor and mental development after one year (Tennes et
al., 1985). The second study suggested THC exposure
through breastmilk in the first month after birth could be
associated with decreased motor development at age one
year (Astley & Little, 1990). Neither study adequately con-
trolled for prenatal exposure to THC.
Finally, breastfeeding encourages maternal behaviour and
bonding between the mother and infant. Maternal consump-
tion of cannabis can compromise mother–infant bonding,
What is the endocannabinoid
system?
The brain produces its own natural
compounds, called endocannabinoids,
which act like THC. Endocannabinoids,
which include anandamide (AEA) and
2-arachidonoylglycerol (2-AG), bind to
cannabinoid (CB1 and CB2) receptors.
Cannabinoid receptors are throughout
the brain and body, meaning that
cannabinoids can influence a broad
range of psychological and biological
processes, such as cognition, emotional
processing and regulation, stress
response, appetite, immune functioning,
the endocrine (hormone) system, sleep
and pain signalling (Zou & Kumar, 2018).
CB1 receptors are more concentrated
in the brain. THC can mimic the activity
of AEA and bind to the CB1 receptors to
exert its psychoactive effects. However,
THC binds CB1 receptors at much
higher levels than AEA, flooding the
endocannabinoid system, leading to
altered functioning of each process.
This flooding means that chronic use of
cannabis (i.e., repeated brain exposure
to THC) can alter the functioning of the
endocannabinoid system, which can
include changes in AEA and 2-AG activity,
and the distribution of cannabinoid
receptors (Jacobson et al., 2019).

Clearing the Smoke on Cannabis: Cannabis Use During Pregnancy and Breastfeeding
13
which may contribute to children’s neurodevelopmental alter-
ations later in life (Best Start Resource Centre, 2017; Shieh
& Kravitz, 2006). For example, recent studies have shown
that postnatal maternal cannabis use was associated with a
shorter breastfeeding duration compared with women who
did not use cannabis postpartum (Crume et al., 2018; Ko
etal., 2018). In addition, because cannabis affects alertness,
understanding and judgment, its use can also comprom-
ise parent–infant interactions (Best Start Resource Centre,
2017; Centre of Excellence for Women’s Health, 2017; Sachs
et al., 2013).
Breastfeeding mothers should also consider harms asso-
ciated with second-hand cannabis smoke, which is espe-
cially harmful for infants and young children (Best Start
Resource Centre, 2017; Centre of Excellence for Women’s
Health, 2017; Colorado Department of Public Health and
Environment, 2017; Wilson et al., 2017). Even though data
on the effects of second-hand cannabis smoke are still
emerging, experts recommend pregnant and breastfeeding
women avoid cannabis smoke as it contains many of the
same harmful chemicals as tobacco smoke, which has the
potential to harm a developing baby (Public Health Agency
of Canada, 2018).
In the absence of sufficient evidence for an association
between cannabis use during lactation and health out-
comes for the infant, using cannabis during lactation is dis-
couraged due to potential risks (Committee on Obstetric
Practice, 2017; Reece-Stremtan & Marinelli, 2015; Society
of Obstetricians and Gynaecologists of Canada, 2022).
Further research is needed to fully evaluate the influence
of cannabis on maternal behaviour and the impact of this
influence on child development and outcomes. In addi-
tion, if women choose to continue using cannabis during
pregnancy, harm reduction strategies such as encouraging
them to use methods of cannabis consumption other than
smoking would be beneficial.
Mechanisms of Action
In the human fetal brain, endogenous cannabinoid CB1
receptors (CB1Rs) are found as early as 14 weeks of gesta-
tion (Biegon & Kerman, 2001), with drastic changes occur-
ring in their expression throughout the gestational period in
different brain areas, notably the limbic structures, which
are involved in emotional regulation (Mato et al., 2003).
Similarly, both endocannabinoids AEA and 2AG are found
in the fetal brain, with concentration levels varying through-
out the perinatal period. That suggests an important role
of the endocannabinoid system during the development of
the fetal brain (Friedrich et al., 2016). Many studies have
confirmed that CB1Rs and endocannabinoids play crucial
roles during fetal development by controlling neurodevelop-
mental processes involved in the development of neurons
and synapses (Berghuis et al., 2007; Harkany et al., 2007;
Maccarrone etal., 2014; Mulder et al., 2008).
The characteristic lipophilic nature of cannabinoids allows
them to cross the placental and blood–brain barrier where
they can activate cannabinoid receptors (Park et al., 2003).
Therefore, exposure to exogenous cannabinoids in utero
may disrupt the fetal endogenous cannabinoid signal-
ling system and consequently the embryo development.
Supporting this idea, a study in humans has shown that
prenatal THC can directly and permanently impair the neur-
onal networks during fetal brain development, an effect
potentially mediated via CB1Rs (Tortoriello et al., 2014).
Studies in humans have also demonstrated that prenatal
cannabis exposure may lead to alterations in various
neurotransmitter (i.e., GABAergic 3, dopaminergic, gluta-
matergic, serotonergic and opioidergic) systems in children
(Fernández-Ruiz et al., 2000; Jutras-Aswad et al., 2009;
Trezza et al., 2008).
Paternal Cannabis Use
Over the years, a growing interest in the effects of prenatal
paternal use of cannabis on offspring has emerged. For
example, the Generation R and ABCD cohorts pinpointed
that paternal cannabis use during the gestational period,
independently of maternal cannabis use, can be associ-
ated with the onset of psychotic-like experiences and other
behavioural disorders in middle childhood (Bolhuis et al.,
2018; Paul et al., 2021). Whether those effects are induced
by epigenetic mechanisms or other underlying etiological
factors remains unclear.
Studies in animals have provided further information about
the long-term effects of paternal cannabis use on offspring:
One study showed that adolescent THC exposure in rats
before mating can lead to lasting behavioural and neuro-
biological abnormalities on the next generation of rats that
have been unexposed to THC. This suggests that THC can
affect parental gametes and have lasting negative effects
on the next generation of rats (Szutorisz et al., 2014).
Supporting this idea, recent evidence coming from human
and animal studies suggested that paternal THC expos-
ure can alter sperm cells’ DNA methylation, therefore influ-
encing offspring genes and development (Murphy et al.,
2018). Another study in rats found that while premating
paternal THC exposure did not have negative effects on
birth weight, survival and growth of the offspring, it induced
long-term attentional and cognitive deficits when offspring
were tested at adolescence (Holloway et al., 2020) or adult-
hood (Levin et al., 2019).

Clearing the Smoke on Cannabis: Cannabis Use During Pregnancy and Breastfeeding
14
Therefore, besides potential direct in utero effects, pre-
natal THC exposure can impact the developing brain
and behaviour via action on gametes, or through epigen-
etic modifications such as DNA methylations or histone
replacement that can modulate gene expression and influ-
ence protein production (Cholewa-Waclaw et al., 2016;
Maze et al., 2014). Further studies need to be conducted
to better understand epigenetic mechanisms potentially
associated with behavioural and developmental disorder
outcomes in offspring exposed to maternal or paternal
cannabis use.
Effects of Cannabidiol During Pregnancy
The effects of CBD use during pregnancy or breastfeeding
are unknown. Both clinical and preclinical studies evaluat-
ing the safety of CBD use during pregnancy are urgently
needed, especially with the widespread belief that CBD can
relieve symptoms associated with pregnancy (i.e., pain,
nausea, vomiting, anxiety).
CBD products often contain THC, which is known to have
negative effects on brain development. There is no clinical
evidence yet about the safety of using CBD during preg-
nancy, and only a few studies on animals have analyzed
the effects of CBD during pregnancy and lactation. For
example, in one older study on rodents, it was shown that
maternal exposure to CBD reduced spermatogenesis and
fertility in male offspring examined at adulthood (Dalterio
& DeRooij, 1986). In a more recent study, Wanner et al.
(2021) found that maternal use of CBD in mice induced
long-term anxiety and cognitive deficits in females but not
in male offspring. These effects were associated with chan-
ges in genes through epigenetic modifications that play
important roles in neuronal function and are known to be
involved in psychiatric and neurodevelopmental disorders.
This preclinical study was the first to identify potential long-
term negative effects induced by maternal prenatal CBD in
female offspring.
Further studies are needed to better evaluate the effects
of CBD use during pregnancy and breastfeeding. While
we are waiting for more robust studies, the Society of
Obstetricians and Gynecologists of Canada (2022) recom-
mended that women should not use cannabis or CBD dur-
ing pregnancy or breastfeeding.
Conclusions and Implications
Brain development involves a complex cascade of events
influenced by prenatal, physical, social and emotional
factors early in life, which can have long-lasting effects
on behaviour (for reviews, see Finnegan, 2013; Leyton &
Stewart, 2014). Maternal cannabis use can directly affect
the prenatal brain and significantly disrupt neural develop-
ment, leading to adverse effects on child development and
brain function, including cognition, emotions and memory
impairments. Cannabis use during pregnancy and breast-
feeding does not appear to be harmless, and there is grow-
ing evidence showing some risks associated with cannabis
use on fetal development. Indeed, the evidence shows that
prenatal cannabis smoking (particularly heavy exposure)
has adverse effects on cognitive functioning, behaviour,
mental health and substance use beginning as early as age
three years and during adolescence.
However, there are some limitations in the available data.
First, many studies do not indicate a gestational age of
exposure, cannabis type, frequency of use, dose and
method of use, and they often rely on self-reported can-
nabis use, which can be inaccurate or underreported. Self-
reports of cannabis should be validated in further studies
using urine toxicology tests.
Conclusions about the effects of prenatal cannabis expos-
ure can be confounded by other maternal risk factors that
tend to occur more frequently in women who use canna-
bis. These factors include lower prenatal care access, poor
nutrition, poor physical and mental health, lower socio-
economic status, lower levels of education and the use
of other substances. Negative perinatal outcomes appear
more pronounced in infants when mothers smoked both
cannabis and tobacco compared with the use of either
substance alone, suggesting an additive effect of using
cannabis with tobacco (Chabarria et al., 2016; El Marroun
et al., 2009). While not yet corroborated by evidence in
humans, animal studies also suggest that cannabis and
alcohol during pregnancy can also have synergistic effects
(Hansen et al., 2008; Seleverstov et al., 2017; Subbanna
et al., 2018).
While prospective longitudinal studies are better able
to assess and adjust for some of these factors to parse
out direct associations with prenatal cannabis exposure,
some other studies do not. Because of the existence of
other potential confounders, the effects of prenatal canna-
bis exposure can be difficult to attribute only to cannabis,
so data should be interpreted with caution. Future stud-
ies should assess and control for confounding variables
that can potentially influence the development of pre-
natally exposed offspring. Additionally, most of the studies
reported only positive correlation or associations between
prenatal cannabis use and offspring negative outcomes.
Positive correlation or association does not mean causal
association. Findings from studies should be interpreted
with caution.

Clearing the Smoke on Cannabis: Cannabis Use During Pregnancy and Breastfeeding
15
Over the years, cannabis THC content from smoked can-
nabis has considerably increased from 3% to 6% in prior
decades to 5% to more than 15% (Hall et al., 2019).
Discrepancies in findings about birth, behavioural and
developmental outcomes among studies might be attrib-
uted to the increasing potency of cannabis over the past
few decades (ElSohly et al., 2016; European Monitoring
Centre for Drugs and Drug Addiction, 2017; University of
Mississippi, National Center for Natural Products Research
[as cited in Executive Office of the President of the United
States, 2013]; Mehmedic et al., 2010). This possibility is
especially relevant for comparisons among the OPPS,
MHPCD and the more recent Generation R studies as the
children enrolled in the latter study may have been exposed
to higher levels of THC.
In addition, authorized retail cannabis stores can be of
concern because of varying THC levels in the available
products. For example, in some cannabis concentrates
made by extracting THC from the plant such as kief, hash
or resin, THC content ranges from 39% to 90%. However,
the legalization of nonmedical cannabis allows consumers
to know exactly the content of the product they are using
and select lower-risk products (e.g., containing less THC).
On the illegal market, there is no guarantee of the THC lev-
els nor any other potentially harmful contaminants. Strong
evidence-based information should be incorporated into
the training of retail cannabis staff, so they can better inform
customers about the potential effects of cannabis use dur-
ing pregnancy and breastfeeding. However, there is no
determined amount of cannabis exposure that is safe. Until
the effects of prenatal cannabis exposure are well under-
stood, the safest option available to pregnant women is to
avoid using cannabis (Best Start Resource Centre, 2017;
Canada FASD Research Network, 2017).
Growing evidence from human and animal studies has
shown that both maternal and paternal cannabis use can
have negative outcomes on offspring neurodevelopment,
and these effects can be linked with the existence of shared
etiological factors, such as genetic and environmental,
familial behaviours, lifestyle habits of the parents and so on.
Further robust clinical studies with both parents along with
increased awareness of potential health outcomes associ-
ated with prenatal cannabis use are crucial to understand-
ing the potential risks of cannabis use during pregnancy.
Cannabis use for therapeutic purposes, including CBD use,
during pregnancy or lactation is also not recommended.
In addition, while consuming cannabis in edible or vapor-
ized forms eliminates the risks of smoking, the child will
still be exposed to the components of cannabis (Colorado
Department of Public Health and Environment, 2017). The
Society of Obstetricians and Gynecologists of Canada (2022)
recommends that women should not use cannabis or CBD
products during pregnancy or breastfeeding. An investment
in public education efforts to increase awareness of the
effects of cannabis use during pregnancy is needed. This
investment would be useful considering that online media
frequently report benefits of cannabis or CBD use that are
not consistent with scientific evidence. Such reports include
the portrayal of cannabis use as helpful for pregnancy symp-
toms, such as morning sickness (Jarlenski et al., 2018).
Implications for Healthcare Professionals
Despite the high prevalence of cannabis use among
women of childbearing age, the potential affect of canna-
bis on the developing brain and the long-term influence on
cognition, behaviour and mental health are still not well-
appreciated by society. Healthcare professionals who pro-
vide care to pregnant women should be well informed of
the latest clinical evidence and research to advise pregnant
women and those of childbearing age of the potential risks.
Healthcare professionals need to explore these issues with
patients and provide unbiased, compassionate information
to women and their partners. Appropriate counselling ser-
vices should also be offered to nursing mothers who are
using cannabis as the benefits of breastfeeding can still
outweigh the possible harms of exposure from occasional
cannabis use (Djulus et al., 2005; Garry et al., 2009).
However, there are growing concerns that the medical
community does not have sufficient guidance for address-
ing maternal cannabis use during pregnancy nor breast-
feeding, and there is a strong need for training in the
management of cannabis use during pregnancy. Improved
communications and guidance from healthcare providers
and resources addressing maternal cannabis use during
pregnancy or breastfeeding are therefore strongly needed.
There is also a need for person-centred, harm reduction
and trauma-informed approaches to discuss cannabis use
during pregnancy and breastfeeding and building a non-
judgmental and trusting relationship between healthcare
providers and pregnant parents.
Prevention efforts aimed at reducing prenatal cannabis
exposure could be aided by clinical guidelines developed for
healthcare practitioners about discussing the health effects
of cannabis use during pregnancy and breastfeeding,
such as those available in Colorado (Colorado Department
of Public Health and Environment, 2017). The Society of
Obstetrician and Gynaecologists of Canada is working on
clinical guidelines that will provide healthcare workers with
the latest evidence on cannabis use and women’s health,

Clearing the Smoke on Cannabis: Cannabis Use During Pregnancy and Breastfeeding
16
with a focus on women who are planning a pregnancy, who
are pregnant or who are breastfeeding.
Implications for Researchers
More research on both maternal and paternal cannabis use
during pregnancy is needed. Knowledge gaps exist about
reporting quantity and quality of cannabis used, CBD effects,
impact of consumption method, timing of use in pregnancy
and effect on breastfeeding. The changing landscape,
including increased accessibility to cannabis, decreased
perceptions of risk, increased THC concentrations in can-
nabis and the advent of potent synthetic cannabinoid prod-
ucts, needs to be examined. Finally, research and preven-
tion efforts should explore the role played by the parental
determinants of health (Brown et al., 2016; Havens et al.,
2009; Passey et al., 2014). Addressing these comorbid con-
ditions needs to be part of a holistic approach to reducing
the risks associated with cannabis use during pregnancy
and breastfeeding.
References
Ansell, E. B., Laws, H. B., Roche, M. J., & Sinha, R. (2015).
Effects of marijuana use on impulsivity and hostility in
daily life. Drug and Alcohol Dependence, 148, 136–142.
https://doi.org/10.1016/j.drugalcdep.2014.12.029
Astley, S. J., & Little, R. E. (1990). Maternal marijuana use
during lactation and infant development at one year.
Neurotoxicology and Teratology, 12(2), 161–168.
https://doi.org/10.1016/0892-0362(90)90129-z
Badowski, S., & Smith, G. (2020). Cannabis use during
pregnancy and postpartum. Canadian Family Physician,
66(2), 98–103.
https://www.cfp.ca/content/cfp/66/2/98.full.pdf
Baker, T., Datta, P., Rewers-Felkins, K., Thompson, H.,
Kallem, R. R., & Hale, T. W. (2018). Transfer of inhaled
cannabis into human breast milk. Obstetrics &
Gynecology. 131(5), 783–788.
https://doi.org/10.1097/AOG.0000000000002575
Bartlett, K., Kaarid, K., Gervais, N., Vu, N., Sharma, S., Patel,
T., & Shea, A. K. (2020). Pregnant Canadians’ perceptions
about the transmission of cannabis in pregnancy and
while breastfeeding and the impact of information from
health care providers on discontinuation of use. Journal of
Obstetrics and Gynaecology Canada, 42(11), 1346–1350.
https://doi.org/10.1016/j.jogc.2020.04.015
Bayrampour, H., Zahradnik, M., Lisonkova, S., & Janssen,
P. (2019). Women’s perspectives about cannabis use
during pregnancy and the postpartum period: An
integrative review.Preventive Medicine,119, 17–23.
https://doi.org/10.1016/j.ypmed.2018.12.002
Beatty, J. R., Svikis, D. S., & Ondersma, S. J. (2012).
Prevalence and perceived financial costs of marijuana
versus tobacco use among urban low-income
pregnant women.Journal of Addiction Research &
Therapy,3(4), Article 1000135.
https://doi.org/10.4172/2155-6105.1000135
Bennett, P., Matheson, I., Notarianni, L. J., Kane, A., &
Reinhardt, D. (1996). Monographs on individual drugs
(Cannabis). In P. N. Bennet (Ed.), Drugs and human
lactation. 2nd ed. (pp. 348–349). Amsterdam, Holland:
Elsevier.
https://doi.org/10.1016/B978-044481981-9/50025-4
Bertrand, K. A., Hanan, N. J., Honerkamp-Smith, G., Best,
B. M., & Chambers, C. D. (2018). Marijuana use by
breastfeeding mothers and cannabinoid concentrations
in breast milk. Pediatrics, 142(3), Article e20181076.
https://doi.org/10.1542/peds.2018-1076
Berghuis, P., Rajnicek, A. M., Morozov, Y. M., Ross, R. A.,
Mulder, J., … Canty, A. (2007). Hardwiring the brain:
Endocannabinoids shape neuronal connectivity.
Science, 316(5828), 1212–1216.
https://doi.org/10.1126/science.1137406
Best Start Resource Centre. (2017). Risks of cannabis on
fertility, pregnancy, breastfeeding and parenting. Toronto,
Ont.: Health Nexus. https://resources.beststart.org/wp-
content/uploads/2019/01/A30-E.pdf
Biegon, A., & Kerman, I. A. (2001). Autoradiographic study of
pre- and postnatal distribution of cannabinoid receptors
in human brain. Neuroimage, 14(6), 1463–1468.
https://doi.org/10.1006/nimg.2001.0939
Bolhuis, K., Kushner, S. A., Yalniz, S., Hillegers, M. H. J.,
Jaddoe, V. W. V., Tiemeier, H., & El Marroun, H. (2018).
Maternal and paternal cannabis use during pregnancy
and the risk of psychotic-like experiences in the
offspring. Schizophrenia Research, 202, 322–327.
https://doi.org/10.1016/j.schres.2018.06.067
Bradley, R. H., & Corwyn, R. F. (2007). Externalizing problems
in fifth grade: Relations with productive activity, maternal
sensitivity, and harsh parenting from infancy through
middle childhood. Developmental Psychology, 43(6),
1390–1401.
https://doi.org/10.1037/0012-1649.43.6.1390
Brown, S. J., Mensah, F. K., Ah Kit, J., Stuart-Butler, D.,
Glover, K., Leane, C., … Yelland, J. (2016). Use of
cannabis during pregnancy and birth outcomes in an
Aboriginal birth cohort: A cross-sectional, population-
based study. BMJ Open, 6(2), Article e010286.
https://doi.org/10.1136/bmjopen-2015-010286
Cadoni, C., Pisanu, A., Solinas, M., Acquas, E., & Chiara,
G. (2001). Behavioural sensitization after repeated
exposure to Δ9-tetrahydrocannabinol and cross-
sensitization with morphine. Psychopharmacology,
158(3), 259–266.
https://doi.org/10.1007/s002130100875

Clearing the Smoke on Cannabis: Cannabis Use During Pregnancy and Breastfeeding
17
Campbell, E. E., Gilliland, J., Dworatzek, P. D. N., De Vrijer,
B., Penava, D., & Seabrook, J. A. (2018). Socioeconomic
status and adverse birth outcomes: A population-based
Canadian sample. Journal of Biosocial Science, 50(1),
102–113. https://doi.org/10.1017/S0021932017000062
Canada FASD Research Network. (2017). Cannabis use
during pregnancy: Effects of cannabis use during
pregnancy. Vancouver, B.C.: Author.
Cannabis. (2021). In Drugs and lactation database (LactMed).
National Library of Medicine (US).
https://www.ncbi.nlm.nih.gov/books/NBK501587/
Centre of Excellence for Women’s Health. (2017). Women
and cannabis. Vancouver, BC: Author.
https://bccewh.bc.ca/wp-content/uploads/2018/03/
InfoSheet-Women-Cannabis0308.pdf
Chabarria, K. C., Racusin, D. A., Antony, K. M., Kahr, M.,
Suter, M. A., Mastrobattista, J. M., & Aagaard, K. M.
(2016). Marijuana use and its effects in pregnancy.
American Journal of Obstetrics & Gynecology, 215(4),
506.e1–506.e7.
https://doi.org/10.1016/j.ajog.2016.05.044
Chang, J. C., Holland, C. L., Tarr, J. A., Rubio, D.,
Rodriguez, K. L., Kraemer, K. L., ... Arnold, R. M.
(2017). Perinatal illicit drug and marijuana use: An
observational study examining prevalence, screening,
and disclosure. American Journal of Health Promotion,
31(1), 35–42.
https://doi.org/10.4278/ajhp.141215-QUAL-625
Chang, J. C., Tarr, J. A., Holland, C. L., De Genna, N. M.,
Richardson, G. A., Rodriguez, K. L., ... Arnold, R. M.
(2019). Beliefs and attitudes regarding prenatal marijuana
use: Perspectives of pregnant women who report use.
Drug and Alcohol Dependence, 196, 14–20.
https://doi.org/10.1016/j.drugalcdep.2018.11.028
Cholewa-Waclaw, J., Bird, A., von Schimmelmann, M.,
Schaefer, A., Yu, H., Song, H., ... Tsai, L.-H. (2016).
The role of epigenetic mechanisms in the regulation
of gene expression in the nervous system. Journal of
Neuroscience, 36(45), 11427–11434.
https://doi.org/10.1523/JNEUROSCI.2492-16.2016
Colorado Department of Public Health and Environment.
(2017). Marijuana pregnancy and breastfeeding guidance
for Colorado health dare providers prenatal visits.
https://www.colorado.gov/pacific/sites/default/files/MJ_
RMEP_Pregnancy-Breastfeeding-Clinical-Guidelines.pdf
Committee on Obstetric Practice. (2017). Committee opinion
no. 722: Marijuana use during pregnancy and lactation.
Obstetrics and Gynecology, 130(4), e205–e209.
https://doi.org/10.1097/AOG.0000000000002354
Conner, S. N., Bedell, V., Lipsey, K., Macones, G. A., Cahill,
A. G., & Tuuli, M. G. (2016). Maternal marijuana use and
adverse neonatal outcomes: A systematic review and
meta-analysis. Obstetrics & Gynecology, 128(4), 713–
723. https://doi.org/10.1097/AOG.0000000000001649
Corsi, D. J., Donelle, J., Sucha, E., Hawken, S., Hsu, H., El-
Chaâr, D., ... Walker, M. (2020). Maternal cannabis use
in pregnancy and child neurodevelopmental outcomes.
Nature Medicine, 26(10), 1536–1540.
https://doi.org/10.1038/s41591-020-1002-5
Corsi, D. J., Hsu, H., Weiss, D., Fell, D. B., & Walker,
M. (2019). Trends and correlates of cannabis use
in pregnancy: A population-based study in Ontario,
Canada from 2012 to 2017. Canadian Journal of Public
Health, 110(1), 76–84.
https://doi.org/10.17269/s41997-018-0148-0
Corsi, D. J., Walsh, L., Weiss, D., Hsu, H., El-Chaar,
D., Hawken, S., Fell, D. B., & Walker, M. (2019).
Association between self-reported prenatal
cannabis use and maternal, perinatal, and neonatal
outcomes.JAMA,322(2), 145–152.
https://doi.org/10.1001/jama.2019.8734
Crume, T. L., Juhl, A. L., Brooks-Russell, A., Hall, K. E.,
Wymore, E., & Borgelt, L. M. (2018). Cannabis use
during the perinatal period in a state with legalized
recreational and medical marijuana: The association
between maternal characteristics, breastfeeding
patterns, and neonatal outcomes. Journal of Pediatrics,
197, 90–96.
https://doi.org/10.1016/j.jpeds.2018.02.005
Dahl, R. E., Scher, M. S., Williamson, D. E., Robles, N.,
& Day, N. (1995). A longitudinal study of prenatal
marijuana use: Effects on sleep and arousal at
age 3 years. Archives of Pediatrics & Adolescent
Medicine, 149(2), 145–150. https://doi.org/10.1001/
archpedi.1995.02170140027004
Dalterio, S. L., & DeRooij, D. G. (1986). Maternal cannabinoid
exposure effects on spermatogenesis in male offspring.
International Journal of Andrology, 9(4), 250–258.
https://doi.org/10.1111/j.1365-2605.1986.tb00888.x
Day, N., Cornelius, M., Goldschmidt, L., Richardson, G.,
Robles, N., & Taylor, P. (1992). The effects of prenatal
tobacco and marijuana use on offspring growth from
birth through 3 years of age. Neurotoxicology and
Teratology, 14(6), 407–414.
https://doi.org/10.1016/0892-0362(92)90051-b
Day, N., Goldschmidt, L., Day, R., Larkby, C., & Richardson,
G. (2015). Prenatal marijuana exposure, age of marijuana
initiation, and the development of psychotic symptoms
in young adults. Psychological Medicine, 45(8), 1779–
1787. https://doi.org/10.1017/S0033291714002906
Day, N. L., Goldschmidt, L., & Thomas, C. A. (2006). Prenatal
marijuana exposure contributes to the prediction of
marijuana use at age 14. Addiction, 101(9), 1313–1322.
https://doi.org/10.1111/j.1360-0443.2006.01523.x
Day, N. L., Leech, S. L., & Goldschmidt, L. (2011). The effects
of prenatal marijuana exposure on delinquent behaviors
are mediated by measures of neurocognitive functioning.
Neurotoxicology and Teratology, 33(1), 129–136.
https://doi.org/10.1016/j.ntt.2010.07.006

Clearing the Smoke on Cannabis: Cannabis Use During Pregnancy and Breastfeeding
18
Day, N. L., Richardson, G. A., Goldschmidt, L., Robles,
N., T., Taylor, P. M., Stoffer, D. S., … Geva, D. (1994).
Effect of prenatal marijuana exposure on the cognitive
development of offspring at age three. Neurotoxicology
and Teratology, 16(2), 169–175.
https://doi.org/10.1016/0892-0362(94)90114-7
Day, N., Sambamoorthi, U., Taylor, P., Richardson, G.,
Robles, N., Jhon, Y., ... Jasperse, D. (1991). Prenatal
marijuana use and neonatal outcome. Neurotoxicology
and Teratology, 13(3), 329–334.
https://doi.org/10.1016/0892-0362(91)90079-c
de Oliveira Silveira, G., Loddi, S., de Oliveira, C. D. R.,
Zucoloto, A. D., Fruchtengarten, L. V. G., & Yonamine,
M. (2017). Headspace solid-phase microextraction
and gas chromatography−mass spectrometry for
determination of cannabinoids in human breast milk.
Forensic Toxicology, 35(1), 125–132.
https://doi.org/10.1007/s11419-016-0346-5
Dickson, B., Mansfield, C., Guiahi, M., Allshouse, A. A.,
Borgelt, L. M., Sheeder, J., … Metz, T. D. (2018).
Recommendations from cannabis dispensaries about
first-trimester cannabis use. Obstetrics and Gynecology,
131(6), 1031–1038.
https://doi.org/10.1097/AOG.0000000000002619
DiNieri, J. A., Wang, X., Szutorisz, H., Spano, S. M., Kaur, J.,
Casaccia, P., ... Hurd, Y. L. (2011). Maternal cannabis
use alters ventral striatal dopamine D2 gene regulation
in the offspring. Biological Psychiatry, 70(8), 763–769.
https://doi.org/10.1016/j.biopsych.2011.06.027
Djulus, J., Moretti, M., & Koren, G. (2005). Marijuana use
and breastfeeding. Canadian Family Physician, 51(3),
349–350. https://www.cfp.ca/content/51/3/349
El Marroun, H. (2010). Prenatal cannabis exposure and infant
development: “A tolerated matter” (Doctoral dissertation).
https://repub.eur.nl/pub/18359/el_marroun_proefschrift.
pdf
El Marroun, H., Bolhuis, K., Franken, I. H., Jaddoe, V. W.
V., Hillegers, M. H., Lahey, B. B., & Tiemeier, H. (2019).
Preconception and prenatal cannabis use and the risk
of behavioural and emotional problems in the offspring;
A multi-informant prospective longitudinal study.
International Journal of Epidemiology, 48(1), 287–296.
https://doi.org/10.1093/ije/dyy186
El Marroun, H., Hudziak, J. J., Tiemeier, H., Creemers,
H., Steegers, E. A., Jaddoe, V. W., … Huizink, A.
C. (2011). Intrauterine cannabis exposure leads to
more aggressive behavior and attention problems in
18-month-old girls. Drug and Alcohol Dependence,
118(2–3), 470–474.
https://doi.org/10.1016/j.drugalcdep.2011.03.004
El Marroun, H., Tiemeier, H., Franken, I. H. A., Jaddoe,
V. W. V., van der Lugt, A., Verhulst, F.C., ... White,
T. (2016). Prenatal cannabis and tobacco exposure
in relation to brain morphology: A prospective
neuroimaging study in young children. Biological
Psychiatry, 79(12), 971–979.
https://doi.org/10.1016/j.biopsych.2015.08.024
El Marroun, H., Tiemeier, H., Steegers, E. A. P., Jaddoe, V. W.
V., Hofman, A., Verhulst, F. C., … Huizink, A. C. (2009).
Intrauterine cannabis exposure affects fetal growth
trajectories: The Generation R Study. Journal of the
American Academy of Child & Adolescent Psychiatry,
48(12), 1173–1181.
https://doi.org/10.1097/CHI.0b013e3181bfa8ee
ElSohly, M. A., Mehmedic, Z., Foster, S., Gon, C., Chandra, S.,
& Church, J. C. (2016). Changes in cannabis potency over
the last 2 decades (1995–2014): Analysis of current data in
the United States. Biological Psychiatry, 79(7), 613–619.
https://doi.org/10.1016/j.biopsych.2016.01.004
European Monitoring Centre for Drugs and Drug Addiction.
(2017). Statistical bulletin 20–7 - Price, purity and
potency. Lisbon, Portugal: Author.
http://www.emcdda.europa.eu/data/stats2017/ppp_en
Executive Office of the President of the United States. (2013).
National Drug Control Strategy: Data supplement 2013
Washington, D.C.: Author.
http://www.obamawhitehouse.gov/sites/default/files/
ondcp/policy-and-research/2013_data_supplement_
final2.pdf
Fernández-Ruiz, J., Berrendero, F., Hernández, M.
L., & Ramos, J. A. (2000). The endogenous
cannabinoid system and brain development. Trends in
Neurosciences, 23(1), 14–20.
https://doi.org/10.1016/s0166-2236(99)01491-5
Finnegan, L. (2013). Licit and illicit drug use during
pregnancy: Maternal, neonatal and early childhood
consequences. Ottawa: Canadian Centre on Substance
Use and Addiction.
https://www.ccsa.ca/sites/default/files/2019-04/CCSA-
Drug-Use-during-Pregnancy-Report-2013-en.pdf
Fried, P. A., & O’Connell, C. M. (1987). A comparison of
the effects of prenatal exposure to tobacco, alcohol,
cannabis and caffeine on birth size and subsequent
growth. Neurotoxicology and Teratology, 9(2), 79–85.
https://doi.org/10.1016/0892-0362(87)90082-1
Fried, P. A., & Watkinson, B. (1990). 36- and 48-month
neurobehavioral follow-up of children prenatally exposed
to marijuana, cigarettes, and alcohol.Journal of
Developmental and Behavioral Pediatrics, 11(2), 49–58.
Fried, P. A., & Watkinson, B. (2000). Visuoperceptual
functioning differs in 9- to 12-year olds prenatally
exposed to cigarettes and marihuana. Neurotoxicology
and Teratology, 22(1), 11–20.
https://doi.org/10.1016/s0892-0362(99)00046-x
Fried, P. A., Watkinson, B., & Gray, R. (1992). A follow-up
study of attentional behavior in 6-year-old children
exposed prenatally to marihuana, cigarettes, and
alcohol. Neurotoxicology and Teratology, 14(5), 299–311.
https://doi.org/10.1016/0892-0362(92)90036-a
Fried, P. A., Watkinson, B., & Gray, R. (1998). Differential
effects on cognitive functioning in 9- to 12-year olds
prenatally exposed to cigarettes and marihuana.
Neurotoxicology and Teratology, 20(3), 293–306.
https://doi.org/10.1016/s0892-0362(97)00091-3

Clearing the Smoke on Cannabis: Cannabis Use During Pregnancy and Breastfeeding
19
Fried, P. A., Watkinson, B., & Gray, R. (2003). Differential
effects on cognitive functioning in 13- to 16-year-
olds prenatally exposed to cigarettes and marihuana.
Neurotoxicology and Teratology, 25(4), 427–436.
https://doi.org/10.1016/s0892-0362(03)00029-1
Fried, P. A., Watkinson, B., & Willan, A. (1984). Marijuana
use during pregnancy and decreased length of
gestation. American Journal of Obstetrics and
Gynecology, 150(1),
23–27.
https://doi.org/10.1016/s0002-9378(84)80103-9
Friedrich, J., Khatib, D., Parsa, K., Santopietro, A., &
Gallicano, G. I. (2016). The grass isn’t always greener:
The effects of cannabis on embryological development.
BMC Pharmacology and Toxicology, 17(1), Article 45.
https://doi.org/10.1186/s40360-016-0085-6
Gabrys, R., & Porath, A.J. (2019). Clearing the smoke
on cannabis: Regular use and cognitive functioning.
Ottawa, Ont.: Canadian Centre on Substance Use and
Addiction.
https://www.ccsa.ca/sites/default/files/2019-09/CCSA-
Cannabis-Use-Cognitive-Effects-Report-2019-en.pdf
Garry, A., Rigourd, V., Amirouche, A., Fauroux, V., Aubry, S., &
Serreau, R. (2009). Cannabis and breastfeeding.Journal
of Toxicology, 2009, Article 596149.
https://doi.org/10.1155/2009/596149
Gartstein, M. A., Bridgett, D. J., Young, B. N., Panksepp, J.,
& Power, T. (2013). Origins of effortful control: Infant and
parent contributions. Infancy, 18(2), 149–183.
https://doi.org/10.1111/j.1532-7078.2012.00119.x
Gluckman, P. D., Hanson, M. A., Cooper, C., & Thornburg,
K. L. (2008). Effect of in utero and early-life conditions
on adult health and disease.New England Journal of
Medicine,359(1), 61–73.
https://doi.org/10.1056/NEJMra0708473
Goldschmidt, L., Day, N. L., & Richardson, G. A. (2000).
Effects of prenatal marijuana exposure on child
behavior problems at age 10.Neurotoxicology and
Teratology,22(3), 325–336.
https://doi.org/10.1016/s0892-0362(00)00066-0
Goldschmidt, L., Richardson, G. A., Cornelius, M. D., & Day,
N. L. (2004). Prenatal marijuana and alcohol exposure
and academic achievement at age 10. Neurotoxicology
and Teratology, 26(4), 521–532.
https://doi.org/10.1016/j.ntt.2004.04.003
Goldschmidt, L., Richardson, G. A., Willford, J., & Day, N.
L. (2008). Prenatal marijuana exposure and intelligence
test performance at age 6. Journal of the American
Academy of Child and Adolescent Psychiatry, 47(1),
254–263.
https://doi.org/10.1097/CHI.0b013e318160b3f0
Goldschmidt, L., Richardson, G. A., Willford, J. A.,
Severtson, S. G., & Day, N. L. (2012). School
achievement in 14-year-old youths prenatally exposed
to marijuana. Neurotoxicology and Teratology, 34(1),
161–167.
https://doi.org/10.1016/j.ntt.2011.08.009
Gray, K. A., Day, N. L., Leech, S., & Richardson, G. A. (2005).
Prenatal marijuana exposure: Effect on child depressive
symptoms at ten years of age. Neurotoxicology and
Teratology, 27(3), 439–448.
https://doi.org/10.1016/j.ntt.2005.03.010
Grewen, K., Salzwedel, A. P., & Gao, W. (2015). Functional
connectivity disruption in neonates with prenatal
marijuana exposure. Frontiers in Human Neuroscience,
9, 601. https://doi.org/10.3389/fnhum.2015.00601
Grywacheski, V., Ali, J., Baker, M. M., Gheorghe, M., Wong,
S. L., & Orpana, H. M. (2021). Opioid and cannabis
use during pregnancy and breastfeeding in relation
to sociodemographics and mental health status: A
descriptive study.Journal of Obstetrics and Gynaecology
Canada,43(3), 329–336.
https://doi.org/10.1016/j.jogc.2020.09.017
Gunn, J. K. L., Rosales, C. B., Center, K. E., Nuñez, A.,
Gibson, S. J., Christ, C., & Ehiri, J. E. (2016). Prenatal
exposure to cannabis and maternal and child health
outcomes: A systematic review and meta-analysis. BMJ
Open, 6(4), Article e009986.
https://doi.org/10.1136/bmjopen-2015-009986
Hall, W., Stjepanovic, D., Caulkins, J., Lynskey, M., Leung,
J., Campbell, G., & Degenhardt, L. (2019). Public health
implications of legalising the production and sale of
cannabis for medicinal and recreational use. The Lancet,
394(10208), 1580–1590. https://doi.org/https://doi.
org/10.1016/S0140-6736(19)31789-1
Hansen, H. H., Krutz, B., Sifringer, M., Stefovska, V., Bittigau,
P., Pragst, F., ... Ikonomidou, C. (2008). Cannabinoids
enhance susceptibility of immature brain to ethanol
neurotoxicity. Annals of Neurology, 64(1), 42–52.
https://doi.org/10.1002/ana.21287
Harkany, T., Guzmán, M., Galve-Roperh, I., Berghuis, P.,
Devi, L. A., & Mackie, K. (2007). The emerging functions
of endocannabinoid signaling during CNS development.
Trends in Pharmacological Sciences, 28(2), 83–92.
https://doi.org/10.1016/j.tips.2006.12.004
Havens, J. R., Simmons, L. A., Shannon, L. M., & Hansen,
W. F. (2009). Factors associated with substance use
during pregnancy: results from a national sample. Drug
and Alcohol Dependence, 99(1–-3), 89–95.
https://doi.org/10.1016/j.drugalcdep.2008.07.010
Hayatbakhsh, M. R., Flenady, V. J., Gibbons, K. S.,
Kingsbury, A. M., Hurrion, E., Mamun, A. A., & Najman,
J. M. (2012). Birth outcomes associated with cannabis
use before and during pregnancy. Pediatric Research,
71(2), 215–219. https://doi.org/10.1038/pr.2011.25
Health Canada. (2021a). Canadian Alcohol and Drugs Survey
(CADS): Summary of results for 2019. Ottawa: Author.
https://www.canada.ca/en/health-canada/services/
canadian-alcohol-drugs-survey/2019-summary.html
Health Canada. (2021b). Canadian Cannabis Survey 2021:
Summary. Ottawa: Author.
https://www.canada.ca/en/health-canada/services/
drugs-medication/cannabis/research-data/canadian-
cannabis-survey-2021-summary.html

Clearing the Smoke on Cannabis: Cannabis Use During Pregnancy and Breastfeeding
20
Health Canada. (2021c). Canadian Cannabis Survey 2020:
Summary. Ottawa: Author.
https://www.canada.ca/en/health-canada/services/
drugs-medication/cannabis/research-data/canadian-
cannabis-survey-2020-summary.html
Holloway, Z. R., Hawkey, A. B., Pippin, E., White, H., Wells,
C., Kenou, B., … Levin, E. D. (2020). Paternal factors in
neurodevelopmental toxicology: THC exposure of male
rats causes long-lasting neurobehavioral effects in their
offspring. NeuroToxicology, 78, 57–63.
https://doi.org/10.1016/j.neuro.2020.01.009
Jacobson, M. R., Watts, J. J., Boileau, I., Tong, J., & Mizrahi,
R. (2019). A systematic review of phytocannabinoid
exposure on the endocannabinoid system: Implications
for psychosis. European Neuropsychopharmacology,
29(3), 330–348.
https://doi.org/10.1016/j.euroneuro.2018.12.014
Jarlenski, M., Koma, J. W., Zank, J., Bodnar, L. M., Tarr, J.
A., & Chang, J. C. (2018). Media portrayal of prenatal
and postpartum marijuana use in an era of scientific
uncertainty. Drug and Alcohol Dependence, 187(1), 116–
122. https://doi.org/10.1016/j.drugalcdep.2018.02.021
Jutras-Aswad, D., DiNieri, J. A., Harkany, T., & Hurd,
Y. L. (2009). Neurobiological consequences of
maternal cannabis on human fetal development and
its neuropsychiatric outcome. European Archives of
Psychiatry and Clinical Neuroscience, 259(7), 395–412.
https://doi.org/10.1007/s00406-009-0027-z
Kharbanda, E. O., Vazquez-Benitez, G., Kunin-Batson, A.,
Nordin, J. D., Olsen, A., & Romitti, P. A. (2020). Birth and
early developmental screening outcomes associated
with cannabis exposure during pregnancy. Journal of
Perinatology, 40(3), 473–480.
https://doi.org/10.1038/s41372-019-0576-6
Ko, J. Y., Tong, V. T., Bombard, J. M., Hayes, D. K., Davy, J.,
& Perham-Hester, K. A. (2018). Marijuana use during and
after pregnancy and association of prenatal use on birth
outcomes: A population-based study. Drug and Alcohol
Dependence, 187(1), 72–78.
https://doi.org/10.1016/j.drugalcdep.2018.02.017
Kochanska, G., & Knaack, A. (2003). Effortful control
as a personality characteristic of young children:
Antecedents, correlates, and consequences. Journal of
Personality, 71(6), 1087–1112.
https://doi.org/10.1111/1467-6494.7106008
Konefal, S., & Porath, A. J. (2019). Clearing the smoke on
cannabis: Regular use and mental health. Ottawa, Ont.:
Canadian Centre on Substance Use and Addiction.
https://www.ccsa.ca/sites/default/files/2019-08/CCSA-
Cannabis-Use-Mental-Health-Report-2019-en_0.pdf
Lee, E., Pluym, I. D., Wong, D., Kwan, L., Varma, V., & Rao,
R. (2020). The impact of state legalization on rates of
marijuana use in pregnancy in a universal drug screening
population. Journal of Maternal-Fetal & Neonatal
Medicine, 1–8.
https://doi.org/10.1080/14767058.2020.1765157
Leech, S. L., Larkby, C. A., Day, R., & Day, N. L. (2006).
Predictors and correlates of high levels of depression
and anxiety symptoms among children at age 10.
Journal of The American Academy of Child and
Adolescent Psychiatry, 45(2), 223–230.
https://doi.org/10.1097/01.chi.0000184930.18552.4d
Leech, S. L., Richardson, G. A., Goldschmidt, L., & Day,
N. L. (1999). Prenatal substance exposure: Effects on
attention and impulsivity of 6-year-olds. Neurotoxicology
and Teratology, 21(2), 109–118.
https://doi.org/10.1016/s0892-0362(98)00042-7
Levin, E. D., Hawkey, A. B., Hall, B. J., Cauley, M., Slade,
S., Yazdani, E., ... Murphy, S. K. (2019). Paternal THC
exposure in rats causes long-lasting neurobehavioral
effects in the offspring. Neurotoxicology and Teratology,
74, Article 106806.
https://doi.org/10.1016/j.ntt.2019.04.003
Leyton, M., & Stewart, S. (Eds.). (2014). Substance abuse
in Canada: Childhood and adolescent pathways to
substance use disorders. Ottawa, Ont.: Canadian
Centre on Substance Use and Addiction.
https://www.ccsa.ca/sites/default/files/2019-04/CCSA-
Child-Adolescent-Substance-Use-Disorders-Report-
2014-en.pdf
Liston, J. (1998). Breastfeeding and the use of recreational
drugs - alcohol, caffeine, nicotine and marijuana.
Breastfeeding Review, 6(2), 27–30.
Luke, S., Hutcheon, J., & Kendall, T. (2019). Cannabis use
in pregnancy in British Columbia and selected birth
outcomes.Journal of Obstetrics and Gynaecology
Canada,41(9), 1311–1317.
https://doi.org/10.1016/j.jogc.2018.11.014
Maccarrone, M., Guzmán, M., Mackie, K., Doherty, P.,
& Harkany, T. (2014). Programming of neural cells
by (endo)cannabinoids: From physiological rules to
emerging therapies. Nature Reviews Neuroscience,
15(12), 786–801. https://doi.org/10.1038/nrn3846
Manning, S., & Drover, A. (2020). Parental perceptions
and patterns of cannabis use during pregnancy and
breastfeeding at a Canadian tertiary obstetrics centre.
Journal of Obstetrics and Gynaecology Canada, 42(5),
681. https://doi.org/10.1016/j.jogc.2020.02.063
Marchei, E., Escuder, D., Pallas, C. R., Garcia-Algar,
O., Gómez, A., Friguls, B., … Pichini, S. (2011).
Simultaneous analysis of frequently used licit and
illicit psychoactive drugs in breast milk by liquid
chromatography tandem mass spectrometry. Journal
of Pharmaceutical and Biomedical Analysis, 55(2),
309–316.
https://doi.org/10.1016/j.jpba.2011.01.028
Mark, K., Gryczynski, J., Axenfeld, E., Schwartz, R. P., &
Terplan, M. (2017). Pregnant women’s current and
intended cannabis use in relation to their views toward
legalization and knowledge of potential harm. Journal of
Addiction Medicine, 11(3), 211–216.
https://doi.org/10.1097/ADM.0000000000000299

Clearing the Smoke on Cannabis: Cannabis Use During Pregnancy and Breastfeeding
21
Mato, S., Del Olmo, E., & Pazos, A. (2003). Ontogenetic
development of cannabinoid receptor expression and
signal transduction functionality in the human brain.
European Journal of Neuroscience, 17(9), 1747–1754.
https://doi.org/10.1046/j.1460-9568.2003.02599.x
Maze, I., Noh, K.-M., Soshnev, A. A., & Allis, C. D. (2014).
Every amino acid matters: Essential contributions
of histone variants to mammalian development and
disease. Nature Reviews Genetics, 15(4), 259–271.
https://doi.org/10.1038/nrg3673
Mehmedic, Z., Chandra, S., Slade, D., Denham, H., Foster,
S., Patel, A. S., ... ElSohly, M. A. (2010). Potency trends
of Δ9-THC and other cannabinoids in confiscated
cannabis preparations from 1993 to 2008. Journal of
Forensic Sciences, 55(5), 1209–1217.
https://doi.org/10.1111/j.1556-4029.2010.01441.x
Merritt, T. A., Wilkinson, B., & Chervenak, C. (2016). Maternal
use of marijuana during pregnancy and lactation:
implications for infant and child development and
their well-being. Academic Journal of Pediatrics and
Neonatology, 2(1), 001–008. https://juniperpublishers.
com/ajpn/pdf/AJPN.MS.ID.555580.pdf
Metz, T. D., & Borgelt, L. M. (2018). Marijuana use in
pregnancy and while breastfeeding. Obstetrics and
Gynecology, 132(5), 1198–1210.
https://doi.org/10.1097/AOG.0000000000002878
Metz, T. D., & Stickrath, E. H. (2015). Marijuana use in
pregnancy and lactation: A review of the evidence.
American Journal of Obstetrics and Gynecology, 213(6),
761–778. https://doi.org/10.1016/j.ajog.2015.05.025
Miller, C. W. (2012). Marijuana use and breastfeeding. Clinical
Lactation, 3(3), 101–107.
https://connect.springerpub.com/content/sgrcl%3A%3A
%3A3%3A%3A%3A3%3A%3A%3A101.full.pdf
Moss, M. J., Bushlin, I., Kazmierczak, S., Koop, D.,
Hendrickson, R. G., Zuckerman, K. E., & Grigsby, T. M.
(2021). Cannabis use and measurement of cannabinoids
in plasma and breast milk of breastfeeding mothers.
Pediatric Research, 90(4), 861–868.
https://doi.org/10.1038/s41390-020-01332-2
Mulder, J., Aguado, T., Keimpema, E., Barabás, K.,
Ballester Rosado, C. J., Nguyen, L., ... Harkany, T.
(2008). Endocannabinoid signaling controls pyramidal
cell specification and long-range axon patterning.
Proceedings of the National Academy of Sciences of the
United States of America, 105(25), 8760–8765.
https://doi.org/10.1073/pnas.0803545105
Murphy, S. K., Itchon-Ramos, N., Visco, Z., Huang, Z.,
Grenier, C., Schrott, R., ... Kollins, S. H. (2018).
Cannabinoid exposure and altered DNA methylation in
rat and human sperm. Epigenetics, 13(12), 1208–1221.
https://doi.org/10.1080/15592294.2018.1554521
National Academies of Sciences, Engineering, and
Medicine. (2017). The health effects of cannabis and
cannabinoids: The current state of evidence and
recommendations for research. Washington, D.C.:
National Academies Press.
https://doi.org/10.17226/24625
Noland, J. S., Singer, L. T., Short, E. J., Minnes, S., Arendt,
R. E., Kirchner, H. L., & Bearer, C. (2005). Prenatal
drug exposure and selective attention in preschoolers.
Neurotoxicology and Teratology, 27(3), 429–438.
https://doi.org/10.1016/j.ntt.2005.02.001
Odom, G. C., Cottler, L. B., Striley, C. W., & Lopez-Quintero,
C. (2020). Perceived risk of weekly cannabis use,
past 30-day cannabis use, and frequency of cannabis
use among pregnant women in the United States.
International Journal of Women’s Health, 12, 1075–
1088. https://doi.org/10.2147/IJWH.S266540
Panlilio, L. V., Zanettini, C., Barnes, C., Solinas, M., &
Goldberg, S. R. (2013). Prior exposure to THC
increases the addictive effects of nicotine in rats.
Neuropsychopharmacology, 38(7), 1198–1208.
https://doi.org/10.1038/npp.2013.16
Park, B., Gibbons, H. M., Mitchell, M. D., & Glassa, M.
(2003). Identification of the CB1 cannabinoid receptor
and fatty acid amide hydrolase (FAAH) in the human
placenta. Placenta, 24(5), 473–478.
https://doi.org/10.1053/plac.2002.0926
Passey, M. E., Sanson-Fisher, R. W., D’Este, C. A., & Stirling,
J. M. (2014). Tobacco, alcohol and cannabis use
during pregnancy: Clustering of risks. Drug and Alcohol
Dependence, 134, 44–50.
https://doi.org/10.1016/j.drugalcdep.2013.09.008
Paul, S. E., Hatoum, A. S., Fine, J. D., Johnson, E. C.,
Hansen, I., Karcher, N. R., ... Bogdan, R. (2021).
Associations between prenatal cannabis exposure and
childhood outcomes: Results from the ABCD study.
JAMA Psychiatry, 78(1), 64–76.
https://doi.org/10.1001/jamapsychiatry.2020.2902
Perez-Reyes, M., & Wall, M. E. (1982). Presence of
Δ9-tetrahydrocannabinol in human milk. New England
Journal of Medicine, 307(13), 819–820.
https://doi.org/10.1056/NEJM198209233071311
Porath, A. J., & Fried, P. A. (2005). Effects of prenatal
cigarette and marijuana exposure on drug use among
offspring. Neurotoxicology and Teratology, 27(2),
267–277. https://doi.org/10.1016/j.ntt.2004.12.003
Public Health Agency of Canada (2018). Thinking about using
cannabis while parenting?
https://www.canada.ca/en/health-canada/services/
drugs-medication/cannabis/health-effects/parents.htm
Reece, A. S., & Hulse, G. K. (2020). Canadian cannabis
consumption and patterns of congenital anomalies:
An ecological geospatial analysis. Journal of Addiction
Medicine, 14(5), e195–e210.
https://doi.org/10.1097/ADM.0000000000000638
Reece-Stremtan, S., Marinelli, K. A. & The Academy of
Breastfeeding Medicine. (2015). ABM clinical protocol
#21: Guidelines for breastfeeding and substance use
or substance use disorder, revised 2015. Breastfeeding
Medicine, 10(3), 135–141.
https://doi.org/10.1089/bfm.2015.9992

Clearing the Smoke on Cannabis: Cannabis Use During Pregnancy and Breastfeeding
22
Renard, J. (2020). Clearing the smoke on cannabis:
Respiratory and cardiovascular effects of cannabis
smoking. Ottawa, Ont.: Canadian Centre on Substance
Use and Addiction. https://www.ccsa.ca/sites/default/
files/2020-10/CCSA-Respiratory-Cardiovascular-Effects-
of-Cannabis-Smoking-Report-2020-en.pdf
Richardson, G. A., Ryan, C., Willford, J., Day, N. L., &
Goldschmidt, L. (2002). Prenatal alcohol and marijuana
exposure: Effects on neuropsychological outcomes at 10
years. Neurotoxicology and Teratology, 24(3), 309–320.
https://doi.org/10.1016/s0892-0362(02)00193-9
Rodriguez, C. E., Sheeder, J., Allshouse, A. A., Scott, S.,
Wymore, E., Hopfer, C., ... Metz, T. D. (2019). Marijuana
use in young mothers and adverse pregnancy outcomes:
A retrospective cohort study. BJOG, 126(12), 1491–
1497. https://doi.org/10.1111/1471-0528.15885
Rompala, G., Nomura, Y., & Hurd, Y. L. (2021). Maternal
cannabis use is associated with suppression of immune
gene networks in placenta and increased anxiety
phenotypes in offspring. Proceedings of the National
Academy of Sciences of the United States of America,
118(47), Article e2106115118.
https://doi.org/10.1073/pnas.2106115118
Sachs, H. C., Committee on Drugs, Frattarelli D. A. C.,
Galinkin, J. L., Green, T. P., Johnson, T., … Van den
Anker, J. (2013). The transfer of drugs and therapeutics
into human breast milk: An update on selected topics.
Pediatrics, 132(3), e796–809.
https://doi.org/10.1542/peds.2013-1985
Schempf, A. H., & Strobino, D. M. (2008). Illicit drug use and
adverse birth outcomes: Is it drugs or context? Journal
of Urban Health, 85(6), Article 858.
https://doi.org/10.1007/s11524-008-9315-6
Schuetze, P., Zhao, J., Eiden, R. D., Shisler, S., & Huestis, M.
A. (2019). Prenatal exposure to tobacco and marijuana
and child autonomic regulation and reactivity: An analysis
of indirect pathways via maternal psychopathology and
parenting. Developmental Psychobiology, 61(7), 1022–
1034. https://doi.org/10.1002/dev.21844
Seleverstov, O., Tobiasz, A., Jackson, J. S., Sullivan, R.,
Ma, D., Sullivan, J. P., ... Bukiya, A. N. (2017). Maternal
alcohol exposure during mid-pregnancy dilates fetal
cerebral arteries via endocannabinoid receptors. Alcohol,
61, 51–61.
https://doi.org/10.1016/j.alcohol.2017.01.014
Shieh, C., & Kravitz, M. (2006). Severity of drug use, initiation of
prenatal care, and maternal-fetal attachment in pregnant
marijuana and cocaine/heroin users. Journal of Obstetric,
Gynecologic, and Neonatal Nursing, 35(4), 499–508.
https://doi.org/10.1111/j.1552-6909.2006.00063.x
Smith, A. M., Fried, P. A., Hogan, M. J., & Cameron, I. (2004).
Effects of prenatal marijuana on response inhibition:
An fMRI study of young adults. Neurotoxicology and
Teratology, 26(4), 533–542.
https://doi.org/10.1016/j.ntt.2004.04.004
Smith, A. M., Fried, P. A., Hogan, M. J., & Cameron, I. (2006).
Effects of prenatal marijuana on visuospatial working
memory: An fMRI study in young adults. Neurotoxicology
and Teratology, 28(2), 286–295.
https://doi.org/10.1016/j.ntt.2005.12.008
Smith, A. M., Mioduszewski, O., Hatchard, T., Byron-
Alhassan, A., Fall, C., & Fried, P. A. (2016). Prenatal
marijuana exposure impacts executive functioning into
young adulthood: An fMRI study. Neurotoxicology and
Teratology, 58, 53–59.
https://doi.org/10.1016/j.ntt.2016.05.010
Sonon, K. E., Richardson, G. A., Cornelius, J. R., Kim, K. H.,
& Day, N. L. (2015). Prenatal marijuana exposure predicts
marijuana use in young adulthood. Neurotoxicology and
Teratology, 47, 10–15.
https://doi.org/10.1016/j.ntt.2014.11.003
Society of Obstetricians and Gynaecologists of Canada.
(2022). Legal cannabis not worth risk for pregnant
women. https://sogc.org/en/content/featured-news/
legal-cannabis-not-work-risk.aspx
Statistics Canada. (2016). Health fact sheets: Low birth
weight newborns in Canada, 2000 to 2013. Ottawa,
Ont.: Author. https://www.statcan.gc.ca/pub/82-
625-x/2016001/article/14674-eng.htm
Statistics Canada. (2019). Canadian Tobacco, Alcohol and
Drugs Survey: Summary of results for 2017. Ottawa,
Ont.: Author.
https://www.canada.ca/en/health-canada/services/
canadian-alcohol-drugs-survey/2017-summary.html
Statistics Canada. (2021). Table 1: Prevalence of cannabis
use in the past three months, by time relative to
legalization and quarter, and selected demographics,
household population aged 15 and older, Canada
(provinces only), first quarters of 2018 and 2019, and
fourth quarter of 2020.National Cannabis Survey.
https://www150.statcan.gc.ca/n1/pub/82-
003-x/2021004/article/00001/tbl/tbl01-eng.htm
Subbanna, S., Nagre, N. N., Shivakumar, M., Joshi, V.,
Psychoyos, D., Kutlar, A., … Basavarajappa, B. S.
(2018). CB1R-mediated activation of caspase-3
causes epigenetic and neurobehavioral abnormalities in
postnatal ethanol-exposed mice. Frontiers in Molecular
Neuroscience, 11, Article 45.
https://doi.org/10.3389/fnmol.2018.00045
Szutorisz, H., DiNieri, J. A., Sweet, E., Egervari, G.,
Michaelides, M., Carter, J. M., ... Hurd, Y. L. (2014).
Parental THC exposure leads to compulsive heroin-
seeking and altered striatal synaptic plasticity in the
subsequent generation. Neuropsychopharmacology,
39(6), 1315–1323.
https://doi.org/10.1038/npp.2013.352
Tennes, K., Avitable, N., Blackard, C., Boyles, C., Hassoun,
B., Holmes, L., & Kreye, M. (1985). Marijuana: Prenatal
and postnatal exposure in the human. NIDA Research
Monograph, 59, 48–60.
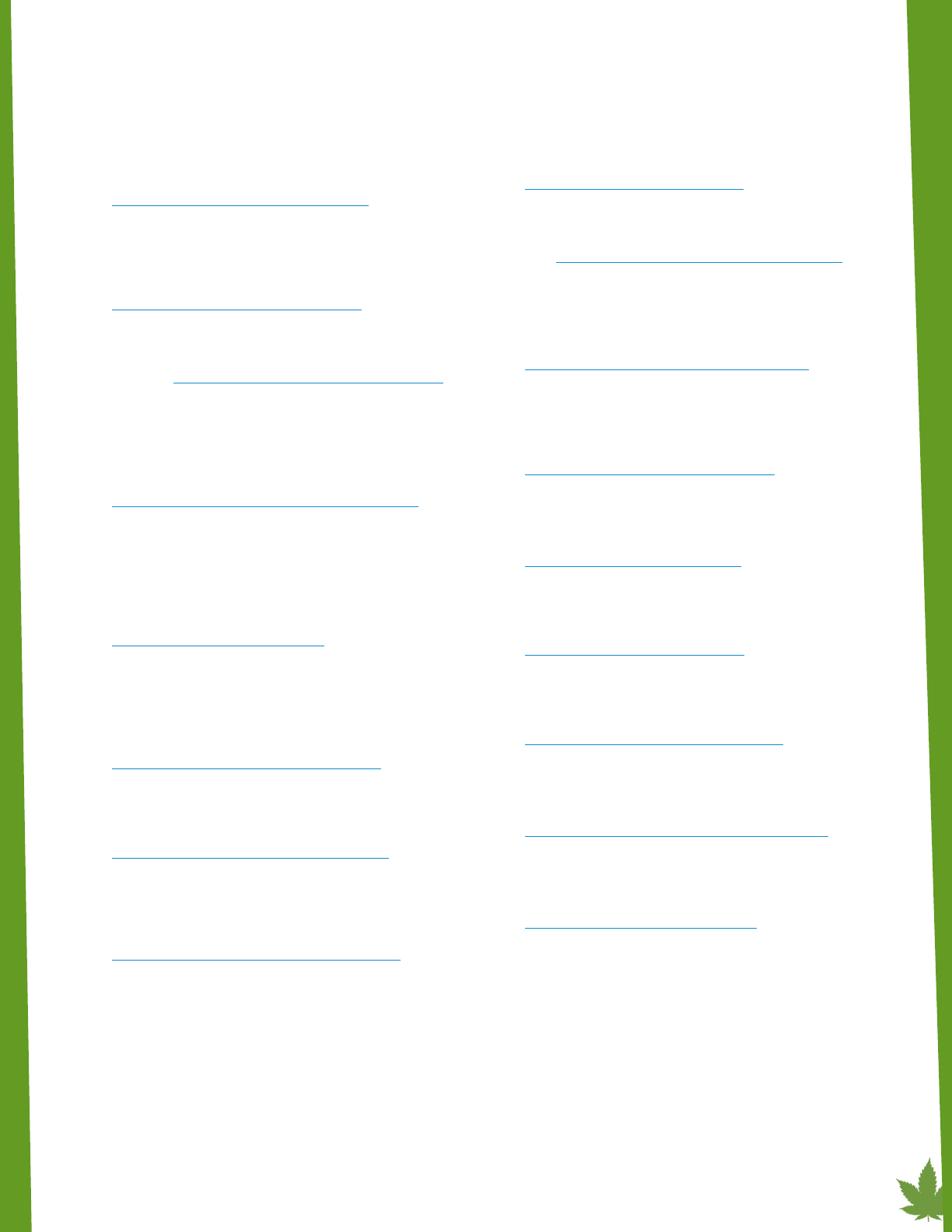
Clearing the Smoke on Cannabis: Cannabis Use During Pregnancy and Breastfeeding
23
Torres, C. A., Medina-Kirchner, C., O’Malley, K. Y., &
Hart, C. L. (2020). Totality of the evidence suggests
prenatal cannabis exposure does not lead to cognitive
impairments: A systematic and critical review. Frontiers in
Psychology, 11, 816.
https://doi.org/10.3389/fpsyg.2020.00816
Tortoriello, G., Morris, C. V., Alpar, A., Fuzik, J., Shirran, S. L.,
Calvigioni, D., ... Harkany, T. (2014). Miswiring the brain:
Δ9-tetrahydrocannabinol disrupts cortical development
by inducing an SCG10/stathmin-2 degradation pathway.
EMBO Journal, 33(7), 668–685.
https://doi.org/10.1002/embj.201386035
Trezza, V., Cuomo, V., & Vanderschuren, L. J. M. J. (2008).
Cannabis and the developing brain: insights from
behavior. European Journal of Pharmacology, 585(2–3),
441–452. https://doi.org/10.1016/j.ejphar.2008.01.058
Turna, J., Belisario, K., Balodis, I., Van Ameringen, M., Busse,
J., & MacKillop, J. (2021). Cannabis use and misuse
in the year following recreational cannabis legalization
in Canada: A longitudinal observational cohort study
of community adults in Ontario.Drug and Alcohol
Dependence,225, Article 108781.
https://doi.org/10.1016/j.drugalcdep.2021.108781
van Gelder, M. M. H. J., Donders, A. R. T., Devine, O.,
Roeleveld, N., Reefhuis, J., & National Birth Defects
Prevention Study (2014). Using Bayesian models to
assess the effects of under-reporting of cannabis use on
the association with birth defects, national birth defects
prevention study, 1997-2005.Paediatric and Perinatal
Epidemiology,28(5), 424–433.
https://doi.org/10.1111/ppe.12140
Velders, F. P., Dieleman, G., Henrichs, J., Jaddoe, V. W.
V., Hofman, A., Verhulst, F. C., ... Tiemeier, H. (2011).
Prenatal and postnatal psychological symptoms of
parents and family functioning: the impact on child
emotional and behavioural problems. European Child &
Adolescent Psychiatry, 20(7), 341–350.
https://doi.org/10.1007/s00787-011-0178-0
Wanner, N. M., Colwell, M., Drown, C., & Faulk, C. (2021).
Developmental cannabidiol exposure increases anxiety
and modifies genome-wide brain DNA methylation in
adult female mice.Clinical Epigenetics,13(1), Article 4.
https://doi.org/10.1186/s13148-020-00993-4
Wang, X., Dow-Edwards, D., Anderson, V., Minkoff, H.,
& Hurd, Y. L. (2004). In utero marijuana exposure
associated with abnormal amygdala dopamine D2 gene
expression in the human fetus. Biological Psychiatry,
56(12), 909–915.
https://doi.org/10.1016/j.biopsych.2004.10.015
Warshak, C. R., Regan, J., Moore, B., Magner, K., Kritzer, S.,
& Van Hook, J. (2015). Association between marijuana
use and adverse obstetrical and neonatal outcomes.
Journal of Perinatology, 35(12), 991–995.
https://doi.org/10.1038/jp.2015.120
Weinsheimer, R. L., & Yanchar, N. L. (2008). Impact of
maternal substance abuse and smoking on children with
gastroschisis. Journal of Pediatric Surgery, 43(5), 879–
883. https://doi.org/10.1016/j.jpedsurg.2007.12.032
Weisbeck, S. J., Bright, K. S., Ginn, C. S., Smith, J. M.,
Hayden, K. A., & Ringham, C. (2021). Perceptions about
cannabis use during pregnancy: A rapid best-framework
qualitative synthesis. Canadian Journal of Public Health
112(1), 49–59.
https://doi.org/10.17269/s41997-020-00346-x
Willford, J. A., Chandler, L. S., Goldschmidt, L., & Day, N.
L. (2010). Effects of prenatal tobacco, alcohol and
marijuana exposure on processing speed, visual–
motor coordination, and interhemispheric transfer.
Neurotoxicology and Teratology, 32(6), 580–588.
https://doi.org/10.1016/j.ntt.2010.06.004
Williams, L. J., Correa, A., & Rasmussen, S. (2004). Maternal
lifestyle factors and risk for ventricular septal defects.
Birth Defects Research. Part A, Clinical and Molecular
Teratology, 70(2), 59–64.
https://doi.org/10.1002/bdra.10145
Wilson, K. M., Torok, M. R., Wei, B., Wang, L., Robinson,
M., Sosnoff, C. S., & Blount, B. C. (2017). Detecting
biomarkers of secondhand marijuana smoke in young
children. Pediatric Research, 81(4), 589–592.
https://doi.org/10.1038/pr.2016.261
Winiger, E. A., & Hewitt, J. K. (2020). Prenatal cannabis
exposure and sleep outcomes in children 9–10 years of
age in the adolescent brain cognitive development SM
study. Sleep Health, 6(6), 787–789.
https://doi.org/10.1016/j.sleh.2020.05.006
Wymore, E. M., Palmer, C., Wang, G. S., Metz, T. D., Bourne,
D. W. A., Sempio, C., & Bunik, M. (2021). Persistence of
Δ-9-tetrahydrocannabinol in human breast milk. JAMA
Pediatrics, 175(6), 632–634.
https://doi.org/10.1001/jamapediatrics.2020.6098
Zou, S., & Kumar, U. (2018). Cannabinoid receptors and
the endocannabinoid system: Signaling and function
in the central nervous system. International Journal of
Molecular Sciences, 19(3), Article 833.
https://doi.org/10.3390/ijms19030833
Acknowledgements
The author thanks the external reviewers for their comments on an earlier version of this report. Production of this docu-
ment has been made possible through a financial contribution from Health Canada. The views expressed herein do
not necessarily represent the views of Health Canada.
ISBN 978-1-77178-960-8 © Canadian Centre on Substance Use and Addiction, 2022.
